CAR-T therapy achieves a 94% overall response rate in relapsed follicular lymphoma — the strongest result of any CAR-T indication to date. In China, the same treatment carries an official list price of roughly $165,000–$185,000, compared to $373,000 in the United States. This guide covers eligibility, leading hospitals, the CAR-T therapy process in China, and how to start your consultation.
Key Facts
- CAR-T therapy (axicabtagene ciloleucel, 奕凯达®) for relapsed/refractory follicular lymphoma carries an official NMPA list price of ¥1.20M (roughly $165,000–$185,000 USD depending on the exchange rate) in China versus $373,000–$600,000+ in the United States as of 2026 — a reduction of more than half.
- The ZUMA-5 trial reported a 94% overall response rate (ORR) and 80% complete response (CR) rate in follicular lymphoma patients — the highest response rates published for any CAR-T indication to date.
- China has 9 NMPA-approved CAR-T products as of July 2026, and is running more than 1,500 registered CAR-T and cellular immunotherapy clinical trials — the largest national portfolio in the world — including studies enrolling patients with indolent B-cell lymphomas.
- CAR-T manufacturing at leading Chinese centers averages 7–21 days vein-to-vein for standard commercial products.
- Axicabtagene ciloleucel (axi-cel, 奕凯达®), developed by Fosun Kite, is the NMPA-approved CD19 CAR-T product specifically indicated for relapsed/refractory follicular lymphoma (3rd line or later) in China.
- Grade 3+ cytokine release syndrome (CRS) occurred in only 7% of FL patients in ZUMA-5 — significantly lower than the 13% rate in DLBCL — making FL one of the safer CAR-T indications from a toxicity standpoint.
- The NCCN guidelines list CD19 CAR-T as a Category 2A recommendation for relapsed/refractory follicular lymphoma after two or more prior lines of therapy.
Table of Contents
Follicular Lymphoma: A Relapsing Disease That CAR-T Can Target
Follicular lymphoma (FL) is the most common indolent B-cell non-Hodgkin lymphoma, accounting for roughly 20–25% of all lymphoma diagnoses globally. It is, by its nature, a disease of relapses and remissions. Standard first-line regimens — typically rituximab-based chemoimmunotherapy such as R-CHOP or R-bendamustine — produce high initial response rates, but the vast majority of patients relapse within five to ten years. Each subsequent line of therapy tends to produce shorter remissions.
For patients who have relapsed after two or more prior lines of therapy, the disease progressively loses its sensitivity to conventional treatment. POD24 (progression of disease within 24 months of initial therapy) is recognized as a high-risk clinical marker; patients who progress early have substantially worse outcomes with standard approaches.
This is exactly the population for which CD19-targeted CAR-T therapy has emerged as a genuinely transformative option.
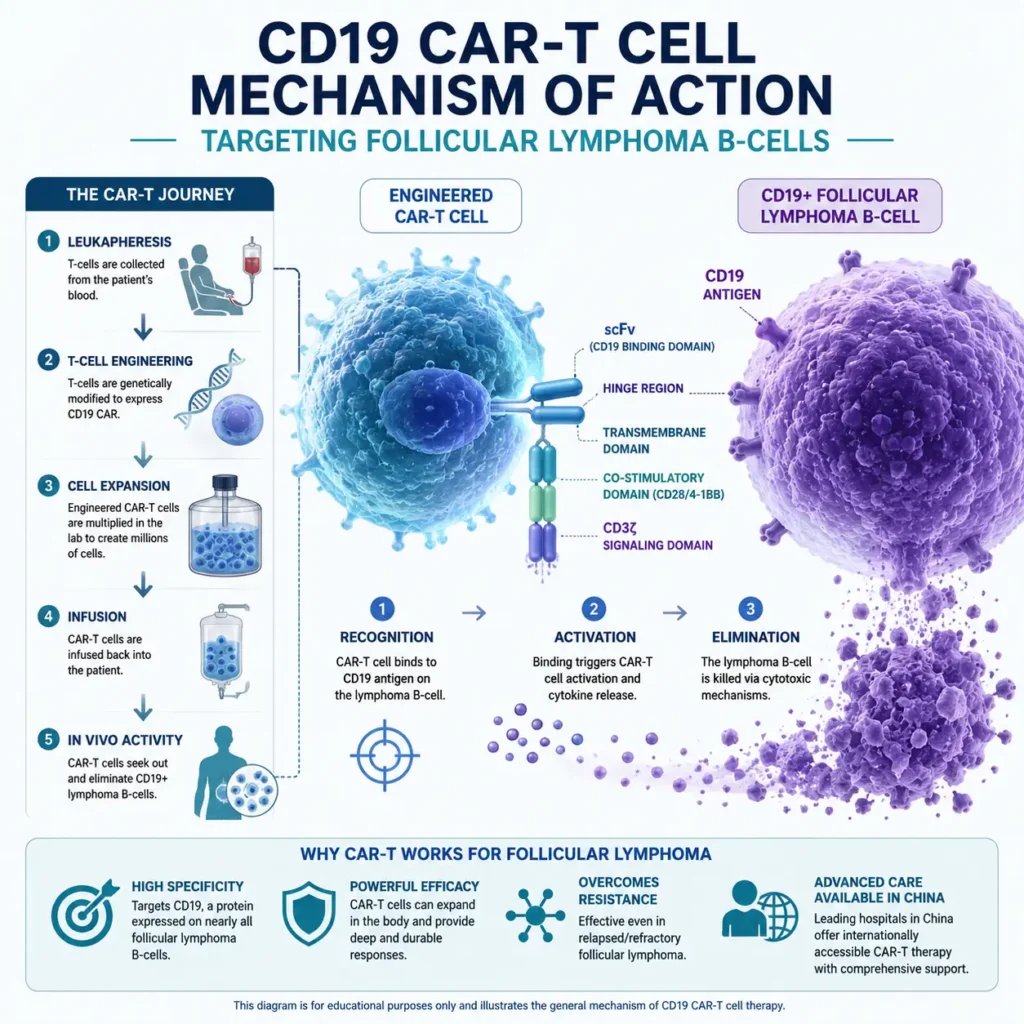
Why FL is particularly well-suited to CD19 CAR-T therapy:
- Follicular lymphoma cells uniformly express CD19 at high, consistent surface density — making them highly susceptible to CD19-directed CAR-T constructs
- FL’s relatively slower proliferation, compared to aggressive lymphomas like DLBCL, means less competing tumor burden pressure on the infused CAR-T cells
- The immunosuppressive tumor microenvironment in FL is less hostile to T-cell persistence than in solid tumors, supporting durable CAR-T engraftment
- Lower tumor proliferation rates also correlate with lower rates of severe cytokine release syndrome (CRS), making FL one of the safer CAR-T indications from a toxicity standpoint
The ZUMA-5 trial — which evaluated axicabtagene ciloleucel (Yescarta) in relapsed/refractory indolent B-cell lymphomas including follicular lymphoma — produced the most striking CAR-T response data published to date: a 94% overall response rate (ORR) and an 80% complete response (CR) rate in FL patients. These are numbers that would be considered exceptional in any oncology context. In a disease historically managed rather than cured, they represent a genuine step-change.
For cancer treatment in China, the accessibility of CAR-T for FL is now a clinical reality — not a distant research prospect.
China’s CAR-T Advantage for Lymphoma
When US oncologists refer patients abroad for CAR-T therapy, cost is the most commonly cited driver — but the clinical case for China goes well beyond price. China has built a CAR-T infrastructure that, for certain indications including follicular lymphoma, now rivals the most advanced Western academic medical centers in both capacity and clinical experience.
The Cost Differential Is Not Marginal
Axicabtagene ciloleucel (Yescarta) carries a list price of $373,000 in the United States — before hospital administration fees, the extended inpatient monitoring period, and the frequently required bridging chemotherapy. For patients without insurance coverage that specifically includes CAR-T (uncommon even among well-insured Americans), the out-of-pocket or financing burden is effectively prohibitive.
In China, axi-cel (奕凯达®) carries an official NMPA list price of ¥1.20M — roughly $165,000–$185,000 USD at leading institutions, depending on the exchange rate — a reduction of more than half. This differential is driven by lower manufacturing labor costs, state-subsidized research hospital infrastructure, and competitive pricing among China’s now nine NMPA-approved domestic CAR-T manufacturers.
Patients interested in CAR-T cell therapy in China should understand that they are not trading quality for cost. The hospitals listed in this guide operate GMP-certified cell manufacturing facilities, carry established international patient departments, and have published peer-reviewed outcome data.
Domestic Chinese CAR-T Products
China is not only administering a Chinese-manufactured version of axi-cel. As of July 2026, the NMPA has approved 9 CAR-T products in total, developed by domestic biotech companies through independent Phase III trials:
| Product | Developer | Indication | NMPA Approval | Official List Price |
|---|---|---|---|---|
| Axi-cel (奕凯达®) | Fosun Kite | r/r large B-cell lymphoma; FL (3rd line+); MCL | Jun 2021 | ¥1.20M (~$165K–$185K) |
| Relma-cel (倍诺达®) | JW Therapeutics (药明巨诺) | r/r large B-cell lymphoma; r/r B-ALL | Sep 2021 | ¥1.29M (~$175K–$200K) |
| Inaticabtagene autoleucel (源瑞达®) | He Yuan Biotech | r/r B-ALL; r/r large B-cell lymphoma | Nov 2023 / Nov 2025 | ¥0.999M (~$135K–$155K) |
| Renialeucel (恒凯莱®) | HRAIN Biotechnology | r/r large B-cell lymphoma (2nd line+) | Jul 2025 | ¥0.89M–¥1.0M (~$120K–$155K) |
| Multiple investigational CD19 constructs | Academic centers | FL, MZL, indolent B-NHLs | Active trial enrollment | Trial-dependent |
Only axi-cel currently carries a specific NMPA-approved follicular lymphoma indication; the other CD19-directed products listed above are approved for large B-cell lymphoma and B-ALL, with FL access at academic centers occurring primarily through clinical trials. The remaining five NMPA-approved CAR-T products target multiple myeloma (BCMA-directed) or, as of June 2026, solid tumors, and are not relevant to follicular lymphoma treatment.
The regulatory environment has been streamlined by the National Medical Products Administration (NMPA) to accelerate approval of domestically developed cell therapies, and the pace of new approvals through 2025–2026 has been significant — China approved five new CAR-T products between late 2024 and mid-2026 alone.
China is currently running more than 1,500 registered CAR-T and cellular immunotherapy clinical trials — the largest national portfolio in the world, including studies of next-generation constructs (bispecific CARs, dual-targeting constructs, armored CARs) for indolent B-cell lymphomas. For international patients arriving in China for the first time, trial enrollment is best treated as a narrow possibility rather than a default plan: research teams typically prioritize patients already under care at the host hospital or referred through established domestic networks, and meeting a trial’s published eligibility criteria does not guarantee a study seat. For most overseas follicular lymphoma patients, one of the nine NMPA-approved commercial CAR-T products remains the realistic starting point. China Care will flag open trial protocols during the initial record review, but cannot guarantee enrollment.
Manufacturing Speed
One underappreciated advantage of China’s CAR-T infrastructure is manufacturing turnaround time. At major centers, the vein-to-vein timeline — from leukapheresis to infusion — runs 7–21 days for standard commercial products. For patients with actively progressing disease who cannot wait weeks for a manufacturing slot, China’s capacity is a meaningful clinical consideration.
Key Hospitals Treating Follicular Lymphoma with CAR-T
The following academic hospitals have established CAR-T programs with specific experience in indolent B-cell lymphomas, including follicular lymphoma. All five maintain international patient departments. A sixth, private specialist option follows for patients who have relapsed after a prior CD19 CAR-T and need dual-target protocols.
1. Institute of Hematology and Blood Diseases Hospital, CAMS — Tianjin
The Institute of Hematology and Blood Diseases Hospital (IHBDH), part of the Chinese Academy of Medical Sciences, is widely considered China’s foremost hematology center. Its CAR-T program is the largest in the country by case volume, with documented experience across B-cell lymphomas including follicular lymphoma, mantle cell lymphoma, and marginal zone lymphoma. The institute operates its own GMP manufacturing facility on-site, enabling some of the shortest vein-to-vein timelines in China. For international patients with complex or heavily pretreated follicular lymphoma, IHBDH represents the highest-acuity referral option in China.
2. Peking University People’s Hospital — Beijing
The Hematology Department at Peking University People’s Hospital is one of the most prolific publishers of CAR-T outcome data in China. The department has conducted trials specifically examining CAR-T in indolent lymphomas, including FL patients who progressed after multiple prior therapies. Its bone marrow transplant unit provides a seamless bridge for patients who may be considered for CAR-T followed by consolidation SCT. The hospital’s international patient center provides English and multilingual support.
3. Ruijin Hospital, Shanghai Jiao Tong University — Shanghai
Ruijin Hospital’s Hematology department is the leading CAR-T center in East China and one of the most active research sites in Asia for cellular immunotherapy. Shanghai’s infrastructure — direct international flights, a large expatriate community, and top-tier hospital hotel facilities — makes it particularly accessible for patients traveling from North America, Europe, or Southeast Asia. Ruijin has enrolled patients from more than 20 countries and operates a dedicated international oncology coordination team.
4. Nanfang Hospital — Guangzhou
Nanfang Hospital’s Hematology and Oncology Center is internationally recognized as a world-class bone marrow transplant and cellular therapy center. Its CAR-T program treats both lymphoma and leukemia patients, and has run clinical trials in indolent B-cell NHLs, though trial seats for first-time overseas patients are limited and not guaranteed. Nanfang is particularly well-positioned for patients traveling from Southeast Asia, given Guangzhou’s direct air connectivity with the region.
5. Sun Yat-sen University Cancer Center (SYSUCC) — Guangzhou
SYSUCC is consistently ranked among China’s top three cancer hospitals and holds a formal partnership with MD Anderson Cancer Center. Its hematology-oncology department treats blood cancers including follicular lymphoma primarily through commercial CAR-T products; SYSUCC also runs an active trial portfolio, but investigational trial access for overseas patients depends on which protocols are open and enrolling at the time, and is not something eligibility alone secures. SYSUCC’s dedicated international oncology coordinator team manages English-language communication, medical record translation, and visa coordination.
6. Beijing GoBroad Hospital — Private Specialist Option
Beijing GoBroad Hospital is a private specialist oncology center in Changping, Beijing, where Dr. Kai Hu’s team has completed over 1,000 CAR-T cases across lymphoma, myeloma, and autoimmune disease. Unlike the five academic centers above, GoBroad is not a public research hospital, and it is best suited to a specific subset of FL patients: those who have already relapsed after a single-target CD19 CAR-T infusion. Dr. Hu’s team has pioneered sequential dual-target constructs (CD19&CD22, CD20&CD22) intended to reduce antigen escape risk in multiply-relapsed cases. For newly relapsed/refractory FL patients who have not yet received CAR-T, one of the five academic centers above remains the more clinically appropriate starting point.
For a broader view of hospital options across China, the China Care hospital directory lists over 50 institutions with hematology and CAR-T capabilities.
Who Qualifies for CAR-T in Follicular Lymphoma?
Patient selection for CAR-T therapy in FL follows criteria similar to those used in major clinical trials, though individual centers apply some flexibility for borderline cases. The following table summarizes the typical eligibility framework:
| Criterion | Standard Requirement | Notes |
|---|---|---|
| Prior lines of therapy | ≥2 prior systemic therapies, including anti-CD20 (rituximab) and alkylating agent | Some trial protocols accept ≥1 prior line with high-risk features (POD24) |
| Disease confirmation | Biopsy-confirmed Grade 1–3a follicular lymphoma; Grade 3b treated as DLBCL protocol | Recent biopsy (within 6 months) preferred |
| Performance status | ECOG 0–2 | ECOG 3 evaluated case-by-case; ECOG 4 typically excluded |
| Cardiac function | LVEF ≥40–50% | Baseline echocardiogram required |
| Renal function | Creatinine clearance ≥40–50 mL/min | Severe renal impairment increases CRS risk |
| Hepatic function | AST/ALT <5× ULN; bilirubin <2× ULN | Active hepatitis B/C requires specialist review |
| Active CNS disease | CNS lymphoma typically excluded from standard protocols | CNS-directed trial protocols exist at select centers |
| Prior CD19-directed therapy | CD19 CAR-T-naive required for CD19 constructs | CD22 or alternate targets available for prior CAR-T failures |
| Bulky disease | Bulky disease (>10cm) manageable but may require bridging therapy | Bridging chemo reduces tumor burden before infusion |
| Active autoimmune disease | Active uncontrolled autoimmune disease typically excluded | Controlled disease on stable immunosuppression evaluated individually |
Patients who received prior CD19-directed therapy (such as an earlier CD19 CAR-T infusion) and relapsed may, in some cases, be evaluated for alternative target constructs (CD22, CD20, bispecific CD19/CD22) under Chinese clinical trial protocols. As of May 2026, investigator-initiated trials of this kind are restricted to public academic hospitals; access depends on the specific protocol open at that center and available enrollment slots at the time, not on meeting the criteria alone.
Watch-and-wait patients who have not yet required systemic therapy are not candidates for CAR-T; treatment is reserved for patients with active disease requiring therapy.
The Treatment Process: Step by Step

Understanding what the CAR-T process involves is essential for planning an international treatment journey. The full timeline from first consultation to discharge typically spans 6–8 weeks.
Step 1: Pre-Treatment Evaluation (Days 1–7)
Upon arrival in China (or prior to travel, via remote record review), the treating hematologist conducts a full staging evaluation: PET/CT scan, bone marrow biopsy if not recent, comprehensive metabolic panel, cardiac echo, pulmonary function if indicated, and infectious disease screening (hepatitis B/C, HIV, CMV status). Medical records from prior therapy lines are reviewed to confirm eligibility and identify bridging needs.
Step 2: Leukapheresis — T-Cell Collection (Day 8–10)
Leukapheresis is a 3–5 hour outpatient procedure in which the patient’s T-lymphocytes are collected via an apheresis machine. The collected cells are then shipped to the manufacturing facility. No sedation is required. Patients may experience mild fatigue; most are ambulatory the same day.
Step 3: Cell Manufacturing (Days 10–24)
The collected T-cells are transduced with a viral vector carrying the CAR gene, then expanded under GMP conditions to produce the therapeutic dose. For standard NMPA-approved commercial products such as axi-cel, manufacturing runs 7–21 days vein-to-vein; the timeline below illustrates a typical case toward the middle of that range. During this period, patients who require disease control may receive bridging chemotherapy (typically bendamustine or low-dose CHOP).
Step 4: Lymphodepletion Chemotherapy (Days 24–27)
Three to four days before CAR-T infusion, patients receive lymphodepleting chemotherapy — most commonly fludarabine plus cyclophosphamide. This conditioning regimen reduces the patient’s existing lymphocyte count and creates physiological space for the incoming CAR-T cells to expand. Patients are admitted to the inpatient hematology unit at this stage.
Step 5: CAR-T Infusion (Day 28)
The infusion itself takes approximately 30–60 minutes and is administered intravenously by the nursing team. There is no procedure-related discomfort during infusion. Patients remain inpatient for monitoring.
Step 6: Monitoring Period (Days 28–42)
The first two weeks following infusion are the critical monitoring window. CAR-T cells begin expanding rapidly in response to CD19-positive tumor cells. The two primary toxicities — cytokine release syndrome (CRS) and immune effector cell-associated neurotoxicity syndrome (ICANS) — typically manifest within this window. The majority of FL patients experience only Grade 1–2 CRS, which resolves with supportive care or tocilizumab. Grade 3+ CRS in FL is significantly less common than in DLBCL — an important distinction for patients concerned about high-intensity toxicity.
Step 7: Response Assessment and Discharge
A PET/CT response assessment is performed approximately 30 days post-infusion. Patients with complete metabolic response (CMR) — the target outcome — may be discharged to outpatient follow-up. Discharge travel is typically cleared 4–6 weeks post-infusion, with the understanding that follow-up labs and imaging at months 3, 6, and 12 are important for monitoring durability.
China Care coordinates all logistics — from pre-travel record review through discharge and post-treatment monitoring communication with the patient’s home oncologist. Contact us to begin a preliminary eligibility assessment before planning travel.
What the Evidence Shows
The evidence base for CAR-T in follicular lymphoma is unusually strong by CAR-T standards. The landmark data comes from the ZUMA-5 trial, with supporting data now emerging from Chinese centers.
ZUMA-5: The Defining Trial
ZUMA-5 evaluated axi-cel (axicabtagene ciloleucel, Yescarta) in 146 patients with relapsed/refractory indolent B-cell non-Hodgkin lymphomas — 124 of whom had follicular lymphoma. All patients had received at least two prior lines of therapy. The primary results:
| Endpoint | FL Subgroup Result |
|---|---|
| Overall Response Rate (ORR) | 94% |
| Complete Response Rate (CR) | 80% |
| Median duration of response | Not yet reached at data cutoff |
| 2-year progression-free survival | ~57% |
| Any-grade CRS | 82% (mostly Grade 1–2) |
| Grade 3+ CRS | 7% |
| Any-grade ICANS | 57% |
| Grade 3+ ICANS | 19% |
The 94% ORR and 80% CR represent the highest response rates published for any CAR-T indication — substantially exceeding results in DLBCL (ORR ~70–85% in ZUMA-1), multiple myeloma, or B-ALL. The biological reason is consistent with FL’s CD19 expression density and lower tumor aggressiveness. Importantly, many of these responses have proven durable, with a proportion of patients maintaining CR beyond 24 months — raising genuine questions about the potential for functional cure in a subset of FL patients.
On toxicity: The Grade 3+ CRS rate of 7% in ZUMA-5’s FL cohort compares favorably to DLBCL data from ZUMA-1 (approximately 13%). FL patients experience meaningful CRS, but the severe-toxicity tail is shorter. The Grade 3+ ICANS rate of 19% is non-trivial and warrants realistic patient counseling — neurological toxicities can include confusion, tremor, or encephalopathy, but are managed with corticosteroids and typically resolve.
Chinese Center Data
Multiple Chinese academic medical centers have published single-arm or expanded-access data for CD19 CAR-T in B-cell lymphomas, including follicular lymphoma subgroup analyses. While prospective FL-specific Chinese trial data remains limited relative to ZUMA-5’s scale, available published data from IHBDH, Ruijin Hospital, and Nanfang Hospital consistently shows ORR figures in the 85–95% range for indolent lymphoma patients — broadly consistent with ZUMA-5. Domestic CAR-T products such as relma-cel (developed by JW Therapeutics) are NMPA-approved for large B-cell lymphoma and B-ALL rather than follicular lymphoma specifically; FL patients at Chinese academic centers are more commonly treated with axi-cel or, where eligible, next-generation investigational constructs under trial protocols.
The NCCN guidelines (reviewed at NCCN.org) now list CD19 CAR-T as a Category 2A recommendation for relapsed/refractory FL after ≥2 prior lines, reflecting the strength of the ZUMA-5 evidence.
Cost Comparison: China vs USA vs UK vs Singapore
| Country | CAR-T Product | Approximate Total Cost (USD) | Notes |
|---|---|---|---|
| USA | Yescarta (axi-cel) | $373,000–$600,000+ | Drug alone $373K; hospital, monitoring, bridging add $100K–$200K+ |
| UK | Yescarta (via NHS) | NHS-covered for eligible patients; private: £300,000+ | NHS access highly restricted; waiting lists can exceed 6 months |
| Singapore | Yescarta / Kymriah | $250,000–$380,000 SGD (~$185,000–$280,000 USD) | MOH subsidy available for citizens/PRs; limited for foreigners |
| China | Axi-cel (奕凯达®) | $165,000–$185,000 USD (¥1.20M official list price) | Includes drug, administration, 2–3 week monitoring; clinical trials lower or no-cost |
For international patients without domestic insurance coverage in the US, UK, or Singapore, China represents a cost saving of roughly $190,000–$415,000 on a single treatment episode — without a meaningful difference in clinical outcome for follicular lymphoma. RMB prices are official NMPA manufacturer list prices and do not fluctuate; USD figures are approximate reference ranges that move with the exchange rate. Patients considering CAR-T therapy for other hematological conditions will find similar cost structures.
The cost figures for China reflect all-in treatment costs at the hospitals listed in this guide — including pre-treatment evaluation, leukapheresis, manufacturing, lymphodepletion, infusion, and the standard 2–3 week inpatient monitoring period. They do not include accommodation, international flights, or travel insurance. China Care provides a detailed cost estimate during the initial consultation phase.
How to Access CAR-T Therapy for Follicular Lymphoma in China

Step 1: Submit Your Medical Records for Remote Review
Begin by completing the contact form on our website. You will be asked to provide recent pathology reports (confirming follicular lymphoma grade and CD19 status), a treatment history summary (prior regimens, dates, responses), current staging scans (PET/CT preferred), and recent blood work. China Care reviews all documentation and conducts a preliminary eligibility assessment within 5–7 business days.
Step 2: Hospital Matching and Specialist Consultation
Based on your specific clinical profile — FL grade, number of prior lines, performance status, geographic preference, and timeline — China Care identifies the most appropriate hospital from the network listed above. A remote pre-consultation with the treating hematologist can often be arranged before you book travel, allowing you to ask clinical questions directly and confirm the treatment plan.
Step 3: Medical Visa Application
International patients traveling to China for treatment beyond 30 days typically require an S2 medical visa. The official invitation letter can only be issued by the licensed treating hospital — China Care coordinates with the hospital to secure it and guides you through the rest of the application. Standard processing at the Chinese Visa Application Service Center is approximately 4 business days once a complete application is submitted. Our comprehensive China medical visa guide covers all documentation requirements, processing options, and the 30-day visa-free exemption that may apply to shorter visits.
Step 4: Travel, Arrival, and Treatment
China Care coordinates airport transfer, hospital registration, interpreter services throughout the treatment period, accommodation recommendations adjacent to the treating hospital, and daily check-ins during the inpatient monitoring phase. A dedicated case coordinator remains your point of contact from arrival to discharge.
Step 5: Discharge and Home Oncologist Communication
At discharge, China Care provides a comprehensive treatment summary in English — including the CAR-T product administered, conditioning regimen, toxicities experienced and managed, response assessment results, and recommended follow-up schedule — formatted for handover to your home oncologist. Follow-up remote consultations with the Chinese treating team are available at months 3, 6, and 12 post-infusion.
To begin the process, contact China Care today. Initial record reviews are provided at no charge.
FAQs
1. My oncologist recommends watch-and-wait for my follicular lymphoma. Should I be considering CAR-T instead?
Watch-and-wait (observation without treatment) remains the appropriate initial approach for asymptomatic, low-tumor-burden follicular lymphoma. CAR-T therapy is not indicated for treatment-naive patients; it is a therapy for relapsed or refractory disease after at least two prior systemic treatment lines. If you are on watch-and-wait, the most important action is to discuss with your oncologist at what point treatment will become necessary, and to document your CD19 status and FL grade accurately so that CAR-T eligibility can be assessed quickly when relapse occurs. Being informed about options — including CAR-T — before you need them is the purpose of guides like this one.
2. What is the risk of Grade 3 or higher CRS in follicular lymphoma patients receiving CAR-T?
In the ZUMA-5 trial, which is the most rigorous published dataset for CAR-T in FL, Grade 3+ CRS occurred in approximately 7% of follicular lymphoma patients. This is meaningfully lower than the 13% Grade 3+ CRS rate observed in DLBCL (ZUMA-1). The lower rate in FL is consistent with the disease’s slower proliferation kinetics, which results in less sudden and intense immune activation. The majority of FL patients receiving CAR-T experience Grade 1–2 CRS — symptoms such as fever, mild hypotension, or oxygen requirement managed with fluids, supportive care, or tocilizumab. Grade 3+ CRS requires ICU-level management, which the hospitals listed in this guide are equipped to provide. ICANS (neurological toxicity) at Grade 3+ occurred in 19% of the ZUMA-5 FL cohort and is a more material consideration; patients should discuss their personal neurological risk profile with the treating hematologist.
3. Is CAR-T therapy for follicular lymphoma considered curative?
CAR-T therapy is not described as curative for follicular lymphoma, and no responsible clinician or facilitation company should represent it as such. What the evidence shows — particularly the ZUMA-5 data — is that a substantial proportion of FL patients achieve durable complete responses extending beyond two years, with ongoing follow-up. Whether long-term complete responses in some patients represent functional cure is a question that requires longer follow-up data. The honest clinical framing is: CAR-T is currently the deepest and most durable treatment option available for relapsed/refractory FL after two or more prior therapies, and a meaningful number of patients will not require further therapy for an extended period.
4. Can I access CAR-T through a clinical trial in China rather than as a commercial product?
It is possible in principle, but international patients should not plan around it. China’s portfolio of active CAR-T clinical trials is the largest in the world, and some studies do enroll follicular lymphoma and other indolent B-cell NHL patients. In practice, however, trial seats are limited and research teams generally prioritize patients already established at that hospital or referred through domestic networks — being medically eligible does not mean a slot is available, and first-time overseas patients are rarely the priority group. China Care will check your records against open protocols as part of the initial assessment and flag any realistic opportunity, but the dependable path for most international patients is one of the nine NMPA-approved commercial CAR-T products. You can also search active studies at ClinicalTrials.gov.
5. How long will I need to stay in China for CAR-T treatment?
Most patients should plan for a total in-country stay of approximately 6–8 weeks. This encompasses the pre-treatment evaluation (approximately 1 week), leukapheresis and the manufacturing wait period (approximately 2 weeks, during which some patients briefly return home if logistics permit), lymphodepletion and infusion (approximately 1 week inpatient), and the post-infusion monitoring period (approximately 2–3 weeks inpatient or closely monitored outpatient). Travel home is typically cleared approximately 4–6 weeks after infusion. Some patients, particularly those requiring bridging therapy or with complex baseline situations, may require a longer stay.
6. Does having a prior autologous stem cell transplant (ASCT) affect CAR-T eligibility?
Prior ASCT does not disqualify a patient from CAR-T therapy. In fact, many patients in the ZUMA-5 trial had received prior ASCT. The key considerations are time since transplant (typically ≥6 months), current lymphocyte count adequate for leukapheresis, absence of active graft-versus-host disease, and organ function within acceptable parameters. Patients who relapsed after ASCT are considered particularly strong CAR-T candidates, as the relapse post-transplant signals limited alternative options with conventional therapy.
7. What happens if CAR-T therapy does not work for my follicular lymphoma?
Non-response to CAR-T in FL (approximately 6% of patients in ZUMA-5 had no response) is uncommon but does occur. Partial response followed by subsequent progression also affects a proportion of patients over time. In these situations, options include re-treatment with CAR-T using a different target (such as CD22 or a dual-target construct), allogeneic stem cell transplant in eligible patients, newer targeted therapies such as PI3K inhibitors, EZH2 inhibitors (tazemetostat), or bispecific antibodies (mosunetuzumab), and — where a matching protocol happens to be open and enrolling — a next-generation CAR-T trial. China’s clinical trial infrastructure means that patients who progress after initial CAR-T may still access further investigational options at the same center. China Care maintains ongoing relationships with treating teams to support post-CAR-T planning.
Start Your Consultation
Relapsed follicular lymphoma has a 94% response rate with CAR-T — at a cost most international patients can access.
China Care Health Tours is a Hong Kong-based medical facilitation service connecting international patients with China’s leading hematology centers for CAR-T therapy. We coordinate every step from record review through post-treatment discharge.
Get a Free Eligibility Assessment →
Learn More About CAR-T Therapy in China →
References
- Wikipedia. “Follicular lymphoma.” Wikipedia. https://en.wikipedia.org/wiki/Follicular_lymphoma
- Jacobson CA, et al. “Axicabtagene Ciloleucel in Relapsed or Refractory Indolent Non-Hodgkin Lymphoma (ZUMA-5 Trial).” Journal of Clinical Oncology, 2022. [clinicaltrials.gov — NCT03105336]
- National Comprehensive Cancer Network (NCCN). “NCCN Clinical Practice Guidelines in Oncology: B-Cell Lymphomas.” NCCN.org. https://www.nccn.org/
- National Medical Products Administration (NMPA). Approval of axicabtagene ciloleucel (奕凯达®) for relapsed/refractory large B-cell lymphoma (June 2021), with subsequent indication expansion to relapsed/refractory follicular lymphoma (3rd line+) and mantle cell lymphoma. NMPA.gov.cn. https://www.nmpa.gov.cn/
- ClinicalTrials.gov. CAR-T cell therapy trials for follicular lymphoma — China-based studies. https://clinicaltrials.gov/
- Institute of Hematology and Blood Diseases Hospital (IHBDH), CAMS. Published outcome data — CD19 CAR-T in indolent B-cell lymphomas including follicular lymphoma subgroup analyses.
- Ruijin Hospital; Nanfang Hospital. Published single-arm CAR-T outcome data for B-cell lymphomas including follicular lymphoma subgroup: ORR 85–95% range consistent with ZUMA-5.