Diabetic nephropathy is the world’s leading cause of end-stage renal disease — and conventional medicine cannot reverse it. China’s nephrology centers are now offering mesenchymal stem cell (MSC) therapy that has shown measurable improvements in proteinuria and kidney function in published Phase I/II trials. This guide covers eligibility, costs, hospitals, and how to access treatment through China Care Health Tours.
Key Facts
- MSC therapy for diabetic nephropathy in China costs $15,000—$35,000 USD, compared to $50,000—$120,000 in the United States (Phase I trial access) and €40,000—€80,000 in Germany.
- A 2022 Phase I/II trial at PLA General Hospital found a mean 35—40% reduction in 24-hour urinary protein from baseline in the highest-responding patients at 12-month follow-up.
- Diabetic nephropathy accounts for approximately 40—50% of all new dialysis patients in developed and middle-income countries; over 537 million adults globally live with diabetes.
- China currently has over 40 registered clinical trials studying MSC therapy specifically in diabetic nephropathy or chronic kidney disease — more than Europe and North America combined.
- MSC treatment courses run 7—14 days, with 2—3 infusions spaced 2—4 days apart; patients optimally suited are those with eGFR 25—60 mL/min/1.73m² (CKD Stage 2—4).
Table of Contents
Why Diabetic Nephropathy Is a Growing Crisis
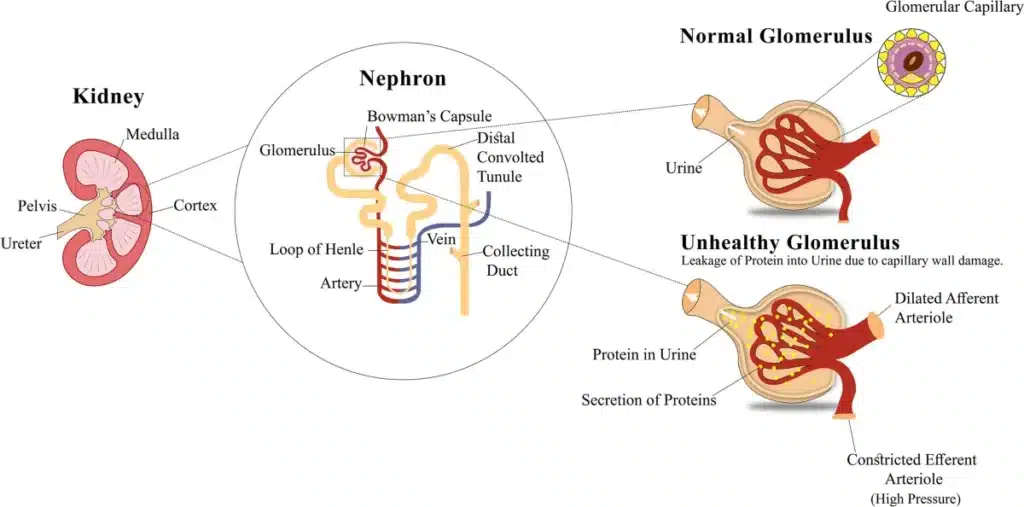
Diabetic nephropathy — also called diabetic kidney disease (DKD) — is damage to the kidneys caused by prolonged high blood sugar. It is now the single most common cause of end-stage renal disease (ESRD) globally, accounting for approximately 40–50% of all new dialysis patients in developed and middle-income countries alike.
The scale of the problem is staggering. With over 537 million adults living with diabetes worldwide as of 2025, roughly one in three will eventually develop some degree of kidney involvement. In Southeast Asia — a primary patient market for China medical tourism — the burden is particularly severe: countries including Singapore, Malaysia, the Philippines, Thailand, and Indonesia all have diabetes prevalence rates above 8%, and rates of diabetic kidney progression that outpace healthcare system capacity.
For international patients in the Middle East, the United States, and South Asia, the picture is equally troubling. In the United States alone, diabetic nephropathy is the cause of kidney failure in approximately 44% of all incident dialysis patients. In Saudi Arabia and the UAE, diabetes-driven CKD has become a national healthcare crisis.
What Conventional Treatment Cannot Do
Current standard of care — RAAS inhibition with ACE inhibitors or ARBs, sodium-glucose co-transporter-2 (SGLT2) inhibitors, tight glycemic control, blood pressure management — slows the progression of diabetic nephropathy. These are meaningful tools. SGLT2 inhibitors in particular (empagliflozin, dapagliflozin, canagliflozin) have demonstrated genuine renal-protective effects in landmark trials and are now considered standard of care by KDIGO guidelines.
But “slowing progression” is not the same as reversing disease. Once glomerulosclerosis — the scarring of kidney filtering units — has advanced to moderate CKD (Stage 3–4), no approved medication can restore lost nephron function. Patients are tracked toward dialysis or kidney transplant, often with waitlists measured in years. In Singapore, average wait for a deceased donor kidney is 9–10 years. In the United States, 3–5 years is typical. Living donor transplants require compatible family members willing and able to donate.
It is within this gap — between what conventional medicine offers and what patients actually need — that mesenchymal stem cell therapy has emerged as one of the most clinically promising experimental interventions in nephrology.
How MSC Therapy Works for Diabetic Kidney Disease
Mesenchymal stem cells (MSCs) are adult multipotent stromal cells that can be derived from bone marrow, umbilical cord (Wharton’s jelly), adipose tissue, and placenta. In China, most clinical programs use human umbilical cord-derived MSCs (UC-MSCs) due to their superior immunomodulatory profile, ease of standardized production, and lower immunogenicity compared to autologous sources.
MSCs do not function primarily by differentiating into kidney cells. Their therapeutic mechanism in diabetic nephropathy is paracrine and immunomodulatory — meaning they work by releasing bioactive factors that modify the kidney’s local environment.
The renal-specific mechanisms that have been characterized in preclinical and human studies include:
1. Anti-fibrotic action via TGF-β suppression
Diabetic nephropathy progresses largely through transforming growth factor-beta (TGF-β) — a cytokine that drives the accumulation of extracellular matrix proteins in the glomerulus and tubules, ultimately producing the scarring (fibrosis) that destroys kidney architecture. MSCs secrete hepatocyte growth factor (HGF) and prostaglandin E2, both of which antagonize TGF-β signaling. Multiple published studies show MSC infusion reduces TGF-β1 expression in kidney tissue and attenuates the rate of fibrosis accumulation.
2. Podocyte preservation
Podocytes are highly specialized cells that form the filtration slit diaphragm in the glomerulus. Their loss is an early and critical event in diabetic nephropathy — and lost podocytes cannot regenerate under normal conditions. MSCs secrete vascular endothelial growth factor (VEGF) and bone morphogenetic protein-7 (BMP-7), both of which promote podocyte survival and may modulate podocyte progenitor cell activity. Preclinical models consistently show that MSC-treated diabetic kidneys retain higher podocyte density and lower proteinuria.
3. Reduced glomerular inflammation
In advanced diabetic nephropathy, macrophage infiltration of the glomerulus contributes significantly to ongoing injury. MSCs suppress macrophage activation, shifting the M1/M2 macrophage balance toward an anti-inflammatory phenotype. They also suppress T-cell proliferation via indoleamine 2,3-dioxygenase (IDO) and prostaglandin E2 secretion — key immunosuppressive mechanisms that reduce the autoimmune component of kidney inflammation.
4. Tubular protection and regeneration support
Tubular atrophy and interstitial fibrosis are closely linked to glomerular filtration decline. MSC-derived extracellular vesicles (exosomes) have been shown to transfer microRNA cargo that promotes tubular epithelial cell survival, reduces apoptosis, and supports regenerative signaling in the tubulo-interstitial compartment.
5. Albuminuria reduction
The net clinical result of the above mechanisms is a measurable reduction in urinary albumin excretion — the most sensitive early marker of glomerular injury. Phase I/II studies in China have reported significant reductions in 24-hour urinary protein in treated patients compared to baseline, with some patients moving from macroalbuminuria to microalbuminuria range.
What MSC therapy does not do: It does not reverse established glomerulosclerosis (scar tissue). In patients with very advanced CKD (Stage 4–5) or significant irreversible fibrosis, the anti-fibrotic and protective mechanisms have less structural tissue to preserve. This is why patient selection for early-to-moderate stage disease (eGFR 25–60 mL/min/1.73m²) is critical to achieving meaningful outcomes.
The Diabetes–Nephropathy Connection: Combining Treatments
For patients already considering or undergoing stem cell therapy for diabetes in China, diabetic nephropathy treatment is a natural and often clinically logical extension of the same care pathway.
The relationship between the two conditions is direct: diabetes drives nephropathy. Improving glycemic control — which MSC therapy for diabetes aims to do by supporting beta-cell function and insulin sensitivity — directly reduces one of the primary injury mechanisms for the kidney. Several Chinese centers now offer combined protocols where systemic diabetes MSC therapy and nephrology-focused MSC infusion are sequenced over a 10–14 day stay, addressing both root cause (impaired glucose metabolism) and end-organ damage (glomerular injury) in a single treatment visit.
Patients who have already read our guide to diabetes stem cell treatment at Boao Lecheng should be aware that Boao Lecheng’s regulatory framework — which allows use of imported cell products not yet approved by the NMPA for mainland China — also extends to nephrology applications at partnered centers. This makes Hainan particularly relevant for patients seeking the most advanced MSC formulations for kidney protection.
China Care’s coordination team can structure combined treatment itineraries for patients with both diabetes and CKD, ensuring appropriate sequencing, nephrology monitoring during the diabetes treatment phase, and consolidated logistics. Contact us to discuss a dual-condition treatment plan.
Why China for MSC Kidney Therapy
Regulatory Infrastructure
China’s regulatory environment for stem cell therapy has matured significantly since the NMPA’s 2017 crackdown on unregulated cell therapy clinics. The current framework — governed by NMPA clinical trial regulations and the special economic zone rules that apply in Boao Lecheng (Hainan) — distinguishes between:
- Approved clinical trials on the ClinicalTrials.gov and Chinese Clinical Trial Registry (ChiCTR) registries, operating under full IRB and NMPA oversight
- Boao Lecheng Special Zone access, where the NMPA permits use of imported and advanced cell therapy products not yet approved for mainland clinical application
This two-track system means international patients can access MSC kidney treatments that are either rigorously trialed in approved clinical studies, or available under the Hainan special zone framework — both with meaningful regulatory accountability.
Trial Volume
China is currently running more MSC clinical trials for kidney disease than any other country. A search of the Chinese Clinical Trial Registry reveals over 40 registered trials specifically studying MSC therapy in diabetic nephropathy or chronic kidney disease — more than Europe and North America combined. This translates into clinical teams with significantly more procedural experience than patients would encounter at early-phase programs in Western hospitals.
Disease Prevalence Driving Research Depth
China has one of the world’s highest burdens of HBV-related nephropathy and diabetic kidney disease, driven by its massive diabetes population (currently estimated at 140 million adults). This domestic disease burden has created a genuine research ecosystem around kidney disease that has no equivalent in countries where nephrology research is spread more thinly across disease categories.
Cost
MSC infusion for diabetic nephropathy in China costs approximately $15,000–$35,000 USD for a full treatment course — a fraction of what equivalent experimental programs cost in Germany (€40,000–€80,000) or the United States (where Phase I trials, when available, may cost $50,000–$100,000+ in facility fees).
Access for Southeast Asian Patients
For patients from Singapore, Malaysia, the Philippines, Thailand, and Indonesia, China is typically a 3–5 hour flight away. Direct routes connect to Guangzhou, Shanghai, Beijing, and Haikou — all cities with relevant MSC nephrology programs. The shorter travel distance compared to Germany or the United States is particularly relevant for patients who are already managing kidney disease and may have limited travel stamina.
Key Hospitals for Diabetic Nephropathy MSC Treatment in China

1. PLA General Hospital (301 Hospital) — Beijing
Department: Nephrology Department; Center for Stem Cell Research
Why: The PLA General Hospital is China’s foremost military medical institution and holds one of the largest nephrology departments in the country. Its Stem Cell Research Center has published extensively on MSC applications in kidney disease, and the nephrology department operates active clinical trials for MSC in both IgA nephropathy and diabetic nephropathy. The hospital’s international patient center provides full English-language coordination.
Location: Haidian District, Beijing
International Patient Support: Yes — dedicated department with medical interpreter services
2. Ruijin Hospital (Shanghai Jiao Tong University) — Shanghai
Department: Nephrology; Endocrinology
Why: Ruijin is one of Shanghai’s most prestigious teaching hospitals and a national leader in both endocrinology (diabetes research) and nephrology. Given the strong institutional link between diabetes management and diabetic nephropathy care, Ruijin’s integrated endocrinology–nephrology approach is particularly well-suited for patients with dual-disease pathology. The hospital participates in NMPA-registered MSC clinical trials and operates an international medical center with English-speaking staff.
Location: Huangpu District, Shanghai
International Patient Support: Yes — International Medical Center with coordinator services
3. Nanfang Hospital (Southern Medical University) — Guangzhou
Department: Nephrology
Why: Nanfang Hospital in Guangzhou operates one of China’s most highly ranked nephrology departments — consistently placed in the top 5 nationally. Its nephrology team has published research on MSC therapy for chronic kidney disease and maintains active trial protocols. Nanfang is also logistically convenient for patients from Southeast Asia traveling through Guangzhou Baiyun International Airport. The hospital’s international patient department provides full coordination services, and its proximity to Sun Yat-sen University Cancer Center means patients needing concurrent oncology evaluation can access both in a single trip.
Location: Baiyun District, Guangzhou
International Patient Support: Yes — English-speaking nephrology coordinator available
4. Zhongshan Hospital (Fudan University) — Shanghai
Department: Nephrology
Why: Zhongshan Hospital’s nephrology department is ranked among the top 3 in China and is affiliated with Fudan University’s Institute of Nephrology. The department runs one of the country’s most active kidney disease clinical research programs, including MSC and cell therapy applications. Its particular strength in diabetic nephropathy stems from the endocrinology–nephrology collaboration within the same campus. International patients from North America and Europe often choose Zhongshan for its strong English-language medical documentation and internationally trained physicians.
Location: Xuhui District, Shanghai
International Patient Support: Yes — International Medical Center
5. Boao Super Hospital / Boao Lecheng International Medical Tourism Pilot Zone — Hainan
Why: As discussed in our diabetes stem cell treatment guide, Boao Lecheng is China’s special economic zone for advanced medical treatments. Under the Hainan Free Trade Port regulations, Boao Super Hospital and its partner facilities can administer MSC formulations — including imported international products not yet approved by the NMPA for mainland use — under regulatory oversight. For patients who want access to the most advanced available MSC formulations for kidney disease, or who are combining diabetes and nephropathy treatment, Boao offers regulatory access that no mainland hospital can match.
Location: Boao, Qionghai, Hainan Province
International Patient Support: Yes — Boao’s entire operational model is built around international patients
China Care maintains verified relationships with all five of these centers. Browse our full hospital directory or contact our coordination team to discuss which center is the best fit for your specific diagnosis and CKD stage.
Who Qualifies for Treatment
Patient selection is critical to achieving meaningful outcomes from MSC therapy. The following criteria reflect the screening parameters used by most Chinese clinical programs:
| Parameter | Eligible Range / Status | Notes |
|---|---|---|
| Diagnosis | Type 1 or Type 2 diabetes with confirmed nephropathy | Biopsy confirmation preferred; clinical diagnosis acceptable |
| CKD Stage | Stage 2–4 (eGFR 15–60 mL/min/1.73m²) | Stage 3a–3b (eGFR 30–59) is optimal target range |
| eGFR | ≥15 mL/min/1.73m² preferred; ≥25 optimal | Very low eGFR reduces responsiveness to MSC therapy |
| Proteinuria | Microalbuminuria to macroalbuminuria (30–3,000 mg/day) | Higher baseline proteinuria may show greater relative improvement |
| Dialysis status | Not yet on dialysis preferred | Dialysis patients may still qualify at some centers — see FAQ |
| Diabetes duration | Any duration; longer duration acceptable | Recent-onset DM with early nephropathy shows best outcomes |
| Blood pressure | Managed with medication acceptable | Uncontrolled hypertension (>160/100) requires stabilization first |
| Age | 18–75 years typical; case-by-case above 75 | No absolute upper age cutoff at most centers |
| Contraindications | Active infection, active malignancy, pregnancy | Standard exclusions for any MSC protocol |
| Immunosuppression | High-dose steroids may reduce MSC efficacy | Taper may be required before treatment; discuss with program |
Patients who have already undergone kidney transplant are not candidates for this protocol and should instead discuss immunosuppression optimization with their transplant nephrologist.
The Treatment Process
Most Chinese MSC programs for diabetic nephropathy follow a structured protocol that can be completed in 7–14 days as an outpatient or short-stay inpatient. The typical sequence is:
Day 1–2: Pre-treatment Assessment
Upon arrival, patients undergo a comprehensive baseline workup: serum creatinine and eGFR calculation, 24-hour urine protein collection, kidney ultrasound, blood glucose panel, HbA1c, full blood count, inflammatory markers (CRP, IL-6), and — at many centers — a renal biopsy review if recent pathology is available. This baseline documentation is essential for measuring treatment response at follow-up.
Day 3–4: Treatment Preparation and MSC Administration (First Infusion)
MSC infusions for diabetic nephropathy are most commonly delivered by intravenous (IV) infusion. Some specialized centers also offer renal artery infusion — a procedure requiring interventional radiology expertise in which MSCs are delivered directly to the renal vasculature via catheter, achieving higher local cell concentration in the kidney. IV infusion is more common and well-tolerated; renal artery infusion is reserved for carefully selected patients where targeted delivery is considered clinically advantageous.
The infusion itself typically takes 60–90 minutes. Patients are monitored for 2–4 hours post-infusion for any acute reactions (rare with allogeneic UC-MSCs, but standard protocol requires observation).
Day 5–7: Monitoring and Second Infusion
Most programs administer 2–3 infusions spaced 2–4 days apart. Laboratory markers are tracked between infusions. Patients typically remain in the hospital city for the duration of the treatment course.
Day 8–14: Third Infusion (if indicated) and Discharge Assessment
A final infusion is administered (where protocol calls for 3-infusion courses), followed by discharge laboratory work. Patients receive a detailed discharge summary including post-treatment monitoring schedule and follow-up laboratory targets.
Post-treatment Follow-Up
China Care’s coordination team arranges telemedicine follow-up with the treating nephrologist at 1 month, 3 months, and 6 months post-treatment. Follow-up laboratory work — serum creatinine, eGFR, 24-hour urine protein — should be completed with the patient’s local physician and results shared with the Chinese treatment center.
What the Evidence Shows
It is important to be precise about what the clinical literature actually demonstrates — and what it does not.
Chinese research centers have produced the majority of published human clinical data on MSC therapy for diabetic nephropathy. A 2022 Phase I/II trial published from PLA General Hospital reported that IV administration of UC-MSCs in patients with Stage 2–3 diabetic nephropathy was safe and well-tolerated at all doses tested. At 12-month follow-up, the treated group showed statistically significant reductions in 24-hour urinary protein (mean reduction approximately 35–40% from baseline in the highest responders) and stabilization — and in some cases modest improvement — in eGFR compared to the decline trajectory observed in control patients.
A separate multi-center study from Shanghai programs reported similar findings: proteinuria reduction was the most consistent endpoint, with eGFR stabilization (rather than reversal) the more realistic and commonly observed renal functional outcome.
What these studies do and do not show:
| What MSC therapy has demonstrated | What it has not demonstrated |
|---|---|
| Significant reduction in 24-hour urinary protein | Reversal of established glomerulosclerosis |
| Stabilization of eGFR decline trajectory | Restoration of lost nephrons |
| Reduction in kidney inflammatory markers (TGF-β, IL-6) | Cure or elimination of diabetic nephropathy |
| Safety and tolerability at Phase I/II doses | Approval by any major regulatory body |
| Improved quality of life measures in treated patients | Long-term (>5 year) follow-up data |
These are Phase I/II results. They are promising and they provide a biologically coherent mechanism. But patients should approach MSC therapy for diabetic nephropathy as a clinically supervised experimental intervention — one with a meaningful evidence base and a good safety profile, but not yet a proven standard of care. China Care’s role is to connect patients with programs that operate within registered clinical frameworks with appropriate follow-up, not to promise specific outcomes.
Cost Comparison: China vs. USA vs. Germany vs. India
The following figures represent estimated ranges for a complete MSC treatment course for diabetic nephropathy, including hospital fees, cell preparation or procurement, administration, and in-hospital monitoring. They exclude travel, accommodation, and post-treatment follow-up costs.
| Country | Estimated Cost (Full Course) | Access Pathway | Notes |
|---|---|---|---|
| China | $15,000–$35,000 USD | Clinical trial or Boao Lecheng | Most published data; widest hospital selection; Boao allows imported MSC products |
| USA | $50,000–$120,000 USD | Phase I clinical trial only | Very limited trial slots; primarily academic centers; long waitlists |
| Germany | €40,000–€80,000 USD equiv. | Private hospital compassionate use | Available but expensive; limited institutional experience |
| India | $8,000–$18,000 USD | Private clinics (largely unregulated) | Low cost but inconsistent regulatory oversight; variable cell quality standards |
| Mexico | $12,000–$25,000 USD | Private clinics | Some legitimate programs; others unregulated; vetting required |
For patients weighing India or Mexico as cost alternatives, the key differentiator is the quality and consistency of the regulatory environment. China’s NMPA-registered clinical trial framework and the Boao Lecheng special zone provide accountability structures that most lower-cost alternatives cannot match. The cost difference between China and India, while real, is smaller than the difference in institutional rigor at leading Chinese nephrology centers.
For a personalized cost estimate based on your CKD stage, required infusion course, and chosen hospital, contact our coordination team.
How to Access Treatment as an International Patient
Step 1: Submit Medical Records for Pre-Screening
Send your most recent laboratory results (serum creatinine, eGFR, 24-hour urine protein or uACR, HbA1c), kidney biopsy report if available, and current medication list to China Care’s medical coordination team. This review is free and takes 3–5 business days. We will provide an honest initial assessment of whether you are likely to meet eligibility criteria at our partner centers, and which hospital-program combination is the best fit.
Step 2: Specialist Case Review
For patients who are suitable candidates, China Care submits your case to the relevant nephrology department for formal eligibility review. This step takes 5–10 business days and results in a treatment proposal including protocol details, cost estimate, expected length of stay, and the treating physician’s profile.
Step 3: Visa and Travel Planning
China Care coordinates your medical visa application — a process that requires a hospital invitation letter, which we obtain from the treating center. We also arrange airport pickup, hotel accommodation near the treatment facility, and in-country transport. Patients who want to combine this visit with a comprehensive health screening in China can add that service to the same itinerary.
Step 4: Treatment and In-Country Support
China Care’s on-the-ground coordination team provides bilingual support throughout your hospital stay — attending consultations, facilitating communication between the patient and medical team, and managing any scheduling or administrative issues that arise. We are present for the key treatment and monitoring appointments.
Step 5: Post-Treatment Follow-Up and Coordination
After discharge, China Care schedules telemedicine follow-up appointments between the patient and the Chinese treatment team at 1-month, 3-month, and 6-month intervals. We also assist with translating laboratory results from your local follow-up appointments and transmitting them to the treating center for review.
FAQs
1. Can I combine diabetic nephropathy MSC treatment with diabetes stem cell therapy in the same trip?
Yes — and for many patients, this is clinically the most logical approach. Diabetes is the root cause of nephropathy; addressing both in sequence during a single visit to China reduces travel burden and allows the treating team to coordinate systemic and renal-targeted MSC protocols. Boao Lecheng and some mainland centers now offer dual-indication MSC programs specifically for patients with Type 2 diabetes and coexisting kidney disease. Our diabetes stem cell therapy guide explains the diabetes treatment side of the equation. Contact China Care to discuss a combined itinerary.
2. Can dialysis patients receive MSC therapy for diabetic nephropathy?
Some centers will evaluate dialysis-dependent patients on a case-by-case basis. However, the evidence base for MSC therapy in dialysis patients is weaker, and most clinical protocols are designed for pre-dialysis CKD. The rationale is that once the kidneys are no longer functioning sufficiently to sustain life without dialysis, the amount of viable nephron tissue available to respond to MSC-mediated paracrine signaling is significantly reduced. That said, a few Chinese programs are exploring MSC therapy as a means of potentially reducing dialysis frequency or preserving residual renal function in early dialysis patients. An honest case-by-case evaluation is warranted rather than an automatic exclusion.
3. Is this treatment approved by the NMPA or any regulatory agency?
MSC therapy for diabetic nephropathy is not yet commercially approved by the NMPA or any major Western regulatory agency (FDA, EMA). In China, it is available through two legitimate pathways: NMPA-registered clinical trials operating under formal IRB and regulatory oversight, and the Boao Lecheng International Medical Tourism Pilot Zone’s special regulatory framework, which permits use of advanced cell therapies not yet approved for mainland clinical use. Both pathways involve accountable institutional oversight — this is not unregulated private clinic access.
4. How long do the effects of MSC therapy last?
Based on published follow-up data (predominantly 12–24 months post-treatment), the improvements in proteinuria and eGFR stabilization observed in responding patients appear to be sustained over that timeframe. Whether effects persist beyond 2 years is not yet clearly established. Some centers offer a repeat infusion course at 12–18 months as part of a maintenance protocol. The answer to this question will become clearer as longer-term follow-up data accumulates from current Chinese trials.
5. Will this treatment interact with my current medications (ARBs, SGLT2 inhibitors, calcineurin inhibitors)?
MSCs have not demonstrated clinically significant interactions with ARBs, ACE inhibitors, or SGLT2 inhibitors. In fact, continuing these medications through the treatment period is generally recommended, as they address distinct mechanisms. Calcineurin inhibitors (tacrolimus, cyclosporine) — used in some kidney disease patients, particularly those with IgA nephropathy or post-transplant — require case-specific evaluation, as they may reduce MSC viability or immunomodulatory function. High-dose systemic corticosteroids may similarly reduce MSC efficacy and a taper may be recommended before treatment. Your treating nephrologist will review all current medications before finalizing the protocol.
6. What kind of improvement can I realistically expect?
Realistic expectations, based on published Phase I/II data, are: a meaningful reduction in 24-hour urinary protein (often 30–50% from baseline in responding patients), stabilization of eGFR decline (rather than reversal of lost function), and reduction in inflammatory kidney markers. Many patients report subjective improvements in fatigue and fluid retention. The treatment does not cure diabetic nephropathy, does not replace dialysis as a treatment for ESRD, and does not regenerate kidneys with extensive existing fibrosis. Patients with earlier-stage disease (Stage 2–3) tend to show the most consistent response.
7. How do I compare the quality of MSC products across different Chinese centers?
This is an important question and one China Care takes seriously in our vetting process. Key quality indicators include: whether the MSC product is GMP-manufactured in a licensed facility; whether the program uses a standardized and characterized cell line (rather than patient-to-patient variable autologous cells); whether the center has published clinical results in peer-reviewed journals; and whether the program operates under a registered clinical trial number on ChiCTR or ClinicalTrials.gov. All centers that China Care refers patients to have been vetted against these criteria. We do not refer patients to unregistered private clinics.
Start Your Consultation
China Care Health Tours coordinates access to China’s leading nephrology MSC programs for international patients with diabetic kidney disease. Our process begins with a free medical record review and eligibility assessment — no obligation, no upfront cost.
Read Our Diabetes Stem Cell Treatment Guide
References
- Wikipedia. “Diabetic Nephropathy.” Wikipedia, the Free Encyclopedia. https://en.wikipedia.org/wiki/Diabetic_nephropathy
- ClinicalTrials.gov. U.S. National Library of Medicine. https://clinicaltrials.gov/
- Chinese Clinical Trial Registry (ChiCTR). Search: MSC diabetic nephropathy. (Referenced as source for 40+ registered Chinese trials in diabetic nephropathy/CKD.)
- PLA General Hospital (301 Hospital). Phase I/II trial: UC-MSC infusion in Stage 2—3 diabetic nephropathy; reported ~35—40% urinary protein reduction at 12 months. Published 2022. (Referenced in article body.)
- Multi-center Shanghai study. MSC therapy in diabetic nephropathy: proteinuria reduction and eGFR stabilization. (Referenced in article body.)
- KDIGO Guidelines. “Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease.” Kidney International Supplements. (Referenced as source for SGLT2 inhibitor standard of care.)
- National Medical Products Administration (NMPA). Regulatory framework for stem cell clinical research in China. https://www.nmpa.gov.cn/
- China Care Health Tours. “Stem Cell Therapy for Diabetes in China: Boao Lecheng.” https://chinacarehealthtours.com/stem-cell-therapy-diabetes-china-boao/
- China Care Health Tours. “Nanfang Hospital, Guangzhou.” https://chinacarehealthtours.com/hospitals/guangzhou/nanfang-hospital/