NK (natural killer) cell therapy is an emerging form of cellular immunotherapy being used in China for solid tumors including liver cancer, lung cancer, and gastric cancer. It works through a different mechanism than CAR-T, carries a lower cytokine release syndrome risk, and can be used allogeneically. Explore cancer treatment in China or contact us to discuss eligibility.
Key Facts
- NK cell therapy in China costs $15,000—$50,000 USD per treatment course, compared to $50,000—$150,000+ USD in the United States where no commercial NK therapy is approved for solid tumors.
- Phase I/II data for hepatocellular carcinoma (HCC) — the most mature solid tumor indication — shows partial responses and disease control rates exceeding 50% in some Chinese trials when NK infusion is combined with TACE or anti-PD-1 therapy.
- As of 2026, China hosts more active NK cell therapy clinical trials than any other country, with hundreds of registered NK and CAR-NK studies targeting liver, lung, gastric, and colorectal cancers.
- NK cell manufacturing takes 1—3 weeks for allogeneic off-the-shelf programs, compared to 4—8 weeks for autologous CAR-T; most treatment courses involve 3—5 infusions over 1—2 weeks.
- NK cells can be used allogeneically (from a donor) without graft-versus-host disease (GvHD) risk — enabling off-the-shelf availability that autologous CAR-T cannot match.
Table of Contents
What Are NK Cells and How Do They Fight Cancer?
Natural killer (NK) cells are a type of cytotoxic lymphocyte — white blood cells that form a critical part of the innate immune system. Unlike T cells, which require prior sensitization and antigen presentation to recognize threats, NK cells are primed from birth to detect and destroy abnormal cells without needing previous exposure to a specific pathogen or tumor antigen.
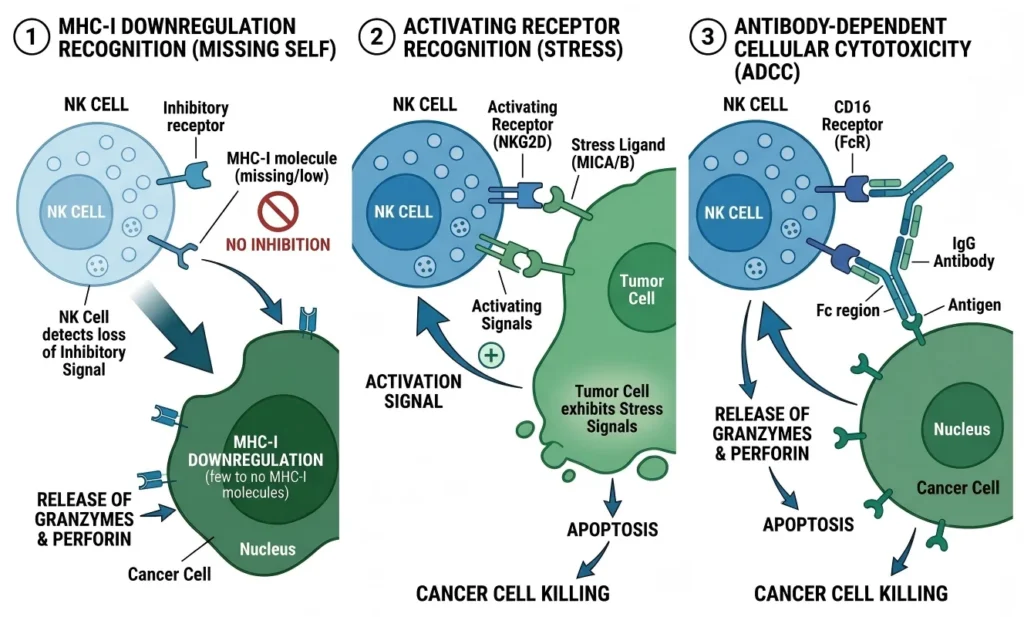
NK cells constantly patrol the body performing a function called immune surveillance: scanning cells for signs of stress, viral infection, or malignant transformation. Their attack mechanism relies on three complementary pathways.
MHC-I Downregulation Recognition
Healthy cells display a surface protein called MHC class I (major histocompatibility complex), which signals to the immune system: “I belong here.” Cancer cells frequently downregulate or lose MHC-I expression — a strategy that allows them to evade T-cell detection. This, however, makes them visible to NK cells. NK cells carry inhibitory receptors (KIRs — killer immunoglobulin-like receptors) that are triggered by healthy MHC-I expression. When MHC-I is absent or reduced, these inhibitory signals are lost, and the NK cell activates and kills.
Activating Receptor Pathways
NK cells also carry activating receptors — including NKG2D, NKp30, NKp44, and NKp46 — that recognize stress ligands expressed on tumor cell surfaces. When these receptors bind their targets on cancer cells, they override any residual inhibitory signals and trigger cytotoxic activity.
ADCC — Antibody-Dependent Cellular Cytotoxicity
NK cells express CD16 (FcγRIII), an Fc receptor that binds the tail of IgG antibodies. When therapeutic monoclonal antibodies (such as trastuzumab, cetuximab, or rituximab) coat a tumor cell, NK cells can recognize the bound antibody via CD16 and destroy the flagged cell — a mechanism called ADCC. This makes NK cells natural partners for antibody-based cancer therapies.
Once activated, NK cells kill tumor cells by releasing cytotoxic granules containing perforin (which punches holes in the target cell membrane) and granzymes (which enter through those holes and trigger apoptosis). NK cells also signal through TRAIL and FasL death ligands, inducing programmed cell death directly.
In clinical NK cell therapy, patient-derived (autologous) or donor-derived (allogeneic) NK cells are collected, expanded ex vivo to large numbers in a laboratory, activated using cytokines such as IL-2, IL-15, or IL-21, and then infused back into the patient. Research programs in China are also engineering NK cell lines (derived from cell line sources such as NK-92) and developing CAR-NK cells — NK cells genetically modified to carry chimeric antigen receptors.
Why NK Cell Therapy for Solid Tumors?
The story of cellular immunotherapy over the past decade has been dominated by CAR-T cell therapy — and for blood cancers (leukemia, lymphoma, multiple myeloma), CAR-T has delivered results that represent a genuine medical breakthrough. But solid tumors have largely resisted CAR-T therapy, and the reasons are structural.
Why CAR-T Struggles with Solid Tumors
CAR-T cells face three compounding obstacles when targeting solid tumors:
- The immunosuppressive tumor microenvironment (TME): Solid tumors generate a biochemical environment rich in immunosuppressive factors — TGF-β, IL-10, adenosine, and PD-L1 expression — that actively exhaust or deactivate infiltrating T cells. CAR-T cells that reach a solid tumor are often rendered non-functional within the tumor mass.
- Antigen heterogeneity: Unlike blood cancers — where CD19, BCMA, or CD22 are expressed uniformly on most malignant cells — solid tumor antigens are heterogeneous. A single CAR-T construct targeting one antigen may eliminate antigen-positive cells while leaving antigen-negative clones to repopulate the tumor.
- Physical trafficking barriers: Solid tumors develop a dense extracellular matrix and abnormal vasculature that physically prevents T cells from infiltrating the tumor in adequate numbers.
NK Cells’ Advantages for Solid Tumors
NK cells do not eliminate all of these obstacles — and it would be misleading to suggest that NK therapy has solved the solid tumor problem that has challenged CAR-T. But NK cells have properties that make them a more naturally suited platform for the solid tumor context:
- MHC-I independence: NK cells do not rely on antigen presentation. This makes them effective against tumor cells that have downregulated or mutated their antigen targets — including cells that have escaped T-cell surveillance precisely because of antigen loss.
- Allogeneic use without GvHD risk: CAR-T cells must generally be autologous (from the patient’s own blood) because donor T cells can attack the patient’s normal tissues — a potentially life-threatening complication called graft-versus-host disease (GvHD). NK cells from healthy donors do not carry the same GvHD risk in the allogeneic setting, which enables off-the-shelf manufacturing, faster treatment timelines, and lower production costs.
- Lower cytokine release syndrome (CRS) risk: CAR-T therapy is associated with potentially severe CRS — a systemic inflammatory response requiring intensive care management. NK cell infusions generally produce less severe cytokine release, making the risk profile more manageable, particularly in patients with compromised performance status.
- Combinability: NK cells work synergistically with monoclonal antibodies (via ADCC), checkpoint inhibitors, and conventional chemotherapy. In China, most clinical NK programs combine NK infusions with one or more of these modalities.
You can read more about the range of cancer treatment options in China across both hematologic and solid tumor settings.
NK Cell Therapy vs CAR-T: Key Differences
NK cell therapy and CAR-T cell therapy are both forms of cellular immunotherapy, but they are distinct in mechanism, risk profile, applicable tumor types, and evidence maturity. Understanding these differences is essential for patients evaluating treatment options.
| Feature | NK Cell Therapy | CAR-T Cell Therapy |
|---|---|---|
| Primary tumor type | Solid tumors (investigational); some blood cancers | Blood cancers (approved); solid tumors (investigational) |
| Mechanism | Innate immune; MHC-I surveillance, activating receptors, ADCC | Adaptive immune; CAR construct targeting specific antigen |
| Cytokine Release Syndrome (CRS) risk | Generally mild to moderate | Can be severe (Grade 3–4), requires ICU capacity |
| Allogeneic feasibility | Yes — lower GvHD risk from donor NK cells | Limited — autologous preferred; allogeneic CAR-T in development |
| Manufacturing time | 1–3 weeks (allogeneic off-the-shelf possible) | 4–8 weeks (autologous requires leukapheresis + engineering) |
| Antigen requirement | Not required — recognizes stress/MHC-I loss patterns | Required — single antigen target per construct |
| Evidence stage | Phase I/II (solid tumors); earlier evidence base | Phase II/III approved (blood cancers); robust data |
| Estimated cost in China | $15,000–$50,000 USD per course | $90,000–$200,000 USD per course |
| Off-the-shelf availability | Yes (allogeneic programs) | Limited |
The key clinical implication: if a patient has a hematologic malignancy (lymphoma, leukemia, multiple myeloma), CAR-T currently has a stronger evidence base and may be the better-supported first-line cellular option. For solid tumor patients — particularly those who have progressed on standard therapy — NK cell therapy represents an active investigational avenue with a different mechanism that may reach tumor cells that have evaded T-cell-based approaches.
For patients considering both modalities, also see our article on CAR-T therapy for autoimmune disease in China, which covers the expanding applications of CAR-T beyond oncology.
Why China Leads in NK Cell Therapy
China’s position in NK cell therapy research is not a coincidence — it reflects sustained institutional investment, favorable regulatory frameworks for early-phase cellular therapy, and manufacturing scale that no other country currently matches.
Clinical Trial Volume
As of 2026, China hosts more active NK cell therapy clinical trials than any other country. A search of ClinicalTrials.gov reveals hundreds of registered NK and CAR-NK studies from Chinese institutions — targeting liver cancer, lung cancer, gastric cancer, colorectal cancer, and other solid tumors, often in combination with established therapies. This trial density means that Chinese patients and international patients accepted into these programs can access therapeutic approaches that are still years from regulatory approval in the United States or Europe.
Regulatory Environment
China’s National Medical Products Administration (NMPA) has established pathways for clinical application of cell therapies in hospital settings that allow academic medical centers to conduct and enroll in NK cell research programs under hospital-level ethics committee approval. This creates a functional route from laboratory to bedside that is faster than the FDA or EMA equivalent at the investigational stage.
Manufacturing Scale and Cost
China’s pharmaceutical manufacturing sector — already the largest in the world by volume — has adapted rapidly to cellular therapy production. GMP-certified cell expansion facilities exist at most major research hospitals, and contract manufacturing organizations (CMOs) with cell therapy capacity have proliferated across the Yangtze River Delta and Pearl River Delta regions. This manufacturing infrastructure allows NK cells to be expanded at far lower cost than in the United States or Germany.

Combination Protocol Experience
Chinese oncologists have accumulated several years of clinical experience combining NK infusions with chemotherapy, PD-1/PD-L1 inhibitors, and interventional procedures such as TACE (transarterial chemoembolization) and RFA (radiofrequency ablation) for liver cancer. The institutional knowledge embedded in these combination protocols is a meaningful clinical asset that is not replicated elsewhere.
Which Hospitals Offer NK Cell Therapy in China?
NK cell therapy programs in China are concentrated in major research hospitals affiliated with national universities and military medical networks. Below are the leading centers with active NK cell programs for solid tumors.
1. PLA General Hospital (301 Hospital), Beijing
PLA General Hospital — formally the Chinese People’s Liberation Army General Hospital — is China’s most comprehensive military and research medical institution, housing over 100 specialty departments. Its Oncology Center and Biological Treatment Research Institute have operated cellular immunotherapy programs for over a decade, including NK cell infusion programs for hepatocellular carcinoma, lung cancer, and gastrointestinal cancers. The hospital’s access to military research funding has allowed it to maintain one of the most technically advanced NK cell expansion programs in China. International patients can access NK therapy through the hospital’s VIP international department, which provides English-language coordination and fast-track specialist access.
2. Sir Run Run Shaw Hospital, Zhejiang University (SAHZU), Hangzhou
Affiliated with Zhejiang University’s School of Medicine, SAHZU is one of eastern China’s leading academic hospitals for oncology research. Its Cancer Center runs active Phase I/II NK cell trials targeting colorectal cancer, lung cancer, and hepatocellular carcinoma, often in combination with anti-PD-1 therapy. SAHZU has a well-established international patient department with English-speaking clinical coordinators, and Hangzhou’s proximity to Shanghai makes logistics relatively accessible for international arrivals.
3. Shanghai Changzheng Hospital
A Tier-3 Grade-A hospital affiliated with the Naval Medical University, Shanghai Changzheng Hospital operates a Hematology and Oncology Center with active NK cell research for solid tumors, including trials combining NK infusion with standard-of-care chemotherapy for advanced gastric and colorectal cancers. Shanghai’s international airport connectivity (both Pudong and Hongqiao) and the city’s established infrastructure for international healthcare visitors make Changzheng Hospital among the more accessible centers on this list.
4. Sun Yat-sen University Cancer Center (SYSUCC), Guangzhou
SYSUCC is consistently ranked among China’s top three cancer hospitals and holds a formal institutional partnership with MD Anderson Cancer Center. While SYSUCC is most internationally recognized for its CAR-T and blood cancer programs, it also runs NK cell immunotherapy research for solid tumors — particularly nasopharyngeal carcinoma (a cancer with unusually high incidence in the Guangdong region) and hepatocellular carcinoma. SYSUCC’s NCCN Global Program membership ensures its protocols align with international oncology standards.
5. Boao Lecheng International Medical Tourism Pilot Zone, Hainan
Boao Lecheng is a unique regulatory zone in Hainan Province that operates under special rules allowing the use of medical technologies not yet commercially approved elsewhere in China. Several hospitals and clinics within the Boao zone — including Boao Super Hospital and affiliated international medical centers — offer NK cell infusion programs as part of integrative oncology packages, often combining NK therapy with other investigational modalities. Boao is particularly attractive for patients who do not meet the enrollment criteria for academic hospital clinical trials, or for those seeking a less intensive initial evaluation. The regulatory freedom of the pilot zone comes with a caveat: program oversight, data collection standards, and clinical rigor vary more widely than at major research hospitals.
Additionally, Nanfang Hospital in Guangzhou has emerging NK cell research programs within its oncology and hematology departments, and should be considered for patients whose tumor type overlaps with its areas of existing strength.
Which Solid Tumors Are Being Treated?
The following table summarizes the solid tumor types currently addressed in China’s NK cell therapy programs, along with the current evidence strength for each indication.
| Tumor Type | Specific Indication | Evidence Strength | Notes |
|---|---|---|---|
| Liver cancer (HCC) | Hepatocellular carcinoma | Strongest for solid tumors | Multiple Phase I/II trials; combination with TACE and anti-PD-1 therapy; most published Chinese data |
| Lung cancer (NSCLC) | Non-small cell lung cancer | Moderate | Phase I/II data; typically used after platinum-based chemotherapy progression |
| Gastric cancer | Advanced gastric / gastroesophageal | Moderate | Combination NK + chemotherapy trials; some responses in heavily pre-treated patients |
| Colorectal cancer (CRC) | Metastatic colorectal | Early-to-moderate | Active trials combining NK with FOLFOX or anti-EGFR antibodies (ADCC mechanism) |
| Pancreatic cancer | Advanced pancreatic ductal adenocarcinoma | Early / investigational | Among the hardest solid tumors; NK research active but responses limited; high unmet need drives trial interest |
| Nasopharyngeal carcinoma (NPC) | Advanced / recurrent NPC | Emerging | Specific to Guangzhou programs; SYSUCC has unique NPC expertise and biobanking |
| Ovarian cancer | Platinum-resistant ovarian | Early | Some NK expansion trials; primarily in combination with bevacizumab |
Important context: The evidence for NK cell therapy in solid tumors is at an earlier stage than the evidence for CAR-T therapy in blood cancers. For blood cancers, CAR-T has achieved response rates of 70–90% in certain settings and has received regulatory approval in both China and the United States. For solid tumors, NK therapy — like CAR-T for solid tumors — is producing promising early results in Phase I/II trials, but has not yet demonstrated the response rates or durability required for approval as standard of care. Patients and families should understand this distinction clearly.
Who Qualifies for NK Cell Therapy?
The following criteria reflect the eligibility parameters used in most Chinese NK cell clinical trial protocols. Patients who do not meet trial eligibility may still access NK therapy through hospital-based compassionate use or Boao Lecheng programs, though these routes require individual assessment.
| Criterion | General Requirement |
|---|---|
| Diagnosis | Histologically confirmed solid tumor (HCC, NSCLC, gastric, colorectal, pancreatic, or NPC preferred) |
| Treatment history | At least one prior line of standard therapy (surgery, chemotherapy, radiation, or targeted therapy) |
| Performance status | ECOG 0–2 (ambulatory; able to travel and tolerate infusion procedure) |
| Organ function | Adequate liver, kidney, and bone marrow function per laboratory criteria |
| Life expectancy | Typically ≥3 months to qualify for trial enrollment |
| Exclusion conditions | Active autoimmune disease; active serious infection; concurrent immunosuppressive therapy (relative, not absolute) |
| Age | Generally 18–75 for trial enrollment; case-by-case for Boao or compassionate use programs |
| HIV / Hepatitis B | Hepatitis B may be acceptable with viral suppression; HIV typically excluded from trials |
Patients who have been told they have “exhausted standard options” are often the most motivated to explore cellular immunotherapy. For such patients, NK therapy’s relatively lower toxicity profile compared to high-dose chemotherapy or some targeted agents makes it a medically reasonable investigational option.
China Care does not determine medical eligibility — eligibility assessment is conducted by the treating oncologists at the selected hospital. Our role is to facilitate the consultation, document translation, and coordination process.
The Treatment Process
NK cell therapy for solid tumors in China is delivered in courses rather than as a single infusion. Understanding the overall process helps patients plan travel, time away from home, and financial preparation.
Phase 1: Medical Record Review (2–3 weeks, remote)
Before any travel, the patient’s oncology records — including pathology reports, imaging (CT/PET-CT/MRI), previous treatment records, and blood work — are translated and submitted to the selected Chinese hospital for pre-screening. China Care coordinates this process. The hospital’s clinical team evaluates whether the patient meets eligibility criteria for a clinical trial or a non-trial NK infusion program. This remote review phase ensures that patients do not travel without reasonable confidence of admission to a program.
Phase 2: Initial In-Country Evaluation (3–5 days, first visit)
The patient travels to China with appropriate medical and travel documentation. Our guide on how to get a medical visa for China covers the visa process in full. On arrival, the hospital conducts a baseline assessment: physical examination, blood panel, tumor marker testing, and imaging if required. The NK cell collection (leukapheresis for autologous programs) or donor cell sourcing (for allogeneic programs) is initiated.
Phase 3: NK Cell Expansion (1–2 weeks)
Collected cells are processed in the hospital’s GMP laboratory. For autologous NK programs, the patient’s own NK cells are expanded and activated using cytokines (IL-2, IL-15, IL-21). For allogeneic programs using donor NK cells or NK cell lines, this phase may be shorter. Patients may remain in-country during this phase or, in some programs, return home and come back for the infusion — depending on the hospital protocol.
Phase 4: Infusion Course (1–2 weeks per course)
NK cell infusions are typically administered intravenously over 30–90 minutes. Most protocols involve 3–5 infusions within a single course, spread over 5–14 days. Patients are monitored post-infusion for cytokine-related symptoms. Compared to CAR-T, serious adverse events are less common, but mild-to-moderate fever, fatigue, and flu-like symptoms are expected.
Phase 5: Response Evaluation and Subsequent Courses
Most NK cell protocols involve 2–4 treatment courses over several months. Response evaluation — CT or PET-CT imaging, tumor marker testing, and clinical assessment — is conducted after each course or every 2 courses. Continued therapy depends on evidence of response or stable disease.

Total Time in China: Most patients should plan for at least one initial stay of 2–3 weeks for the first course (evaluation + cell expansion + first infusion series), and then subsequent visits of 1–2 weeks per course. Patients traveling from Southeast Asia, the Middle East, or within Asia often find the travel burden more manageable than patients from North America or Europe, where long-haul flights add to the physical and logistical challenge.
What the Evidence Shows
Transparency matters — particularly on a YMYL medical topic where patients are making significant decisions. The honest summary of NK cell therapy evidence for solid tumors in 2026 is this: it is real, it is active, and it is promising — but it is not yet a proven standard of care.
What the data supports:
- Phase I trials (primarily in China, Japan, and the United States) have consistently demonstrated that NK cell infusions — both autologous and allogeneic — are feasible and generally well-tolerated in solid tumor patients. Severe adverse events related to the NK therapy itself (as distinct from combination chemotherapy) are uncommon.
- Phase I/II data for hepatocellular carcinoma (HCC) is the most mature for solid tumors, with several Chinese studies showing partial responses and disease stabilization in patients who had progressed on prior therapy, particularly when NK infusion is combined with TACE, sorafenib, or anti-PD-1 checkpoint inhibitors.
- Data for lung cancer (NSCLC) and colorectal cancer shows early signals of activity — disease control rates in some trials exceeding 50% in heavily pre-treated populations — but long-term data on overall survival benefit is not yet available.
- CAR-NK cell constructs (NK cells engineered with CARs targeting HER2, GPC3, or mesothelin for solid tumors) are at the earliest investigational stage and should be distinguished from more established NK expansion-and-infusion approaches.
What the data does not yet support:
- Randomized Phase III trial data demonstrating survival benefit over standard of care (for any solid tumor indication)
- Regulatory approval in any country as standard-of-care treatment for solid tumors
- Reliable prediction of which patients will respond vs. not respond
Why patients still pursue it:
For patients with advanced solid tumors who have exhausted or declined standard therapy options, the calculus is different. When the alternative is best supportive care alone, the risk-benefit assessment of an investigational NK therapy with a manageable safety profile can be rationally favorable — particularly when pursued within a properly supervised clinical trial or hospital-based research program that includes adequate monitoring and follow-up.
China Care facilitates access to this category of treatment. We do not represent NK cell therapy as curative or as a replacement for proven oncology protocols. We represent it as a real investigational option, with real science behind it, being pursued at serious academic institutions — and we help patients access it safely and with full information.
Cost Comparison: China vs USA vs Japan vs Germany
NK cell therapy costs vary significantly across countries, driven by manufacturing infrastructure, regulatory status (trial vs. commercial), and healthcare system economics.
| Country | Cost per Treatment Course | Notes |
|---|---|---|
| China | $15,000–$50,000 USD | Per course; clinical trial enrollment may reduce cost; allogeneic programs at lower end; autologous at higher end |
| USA | $50,000–$150,000+ USD | Primarily in clinical trial settings; commercial NK therapy not approved; significant ancillary costs |
| Japan | $30,000–$80,000 USD | Advanced Therapies Act allows NK therapy in certified hospitals; regulated but expensive; strong HCC program data |
| Germany | $40,000–$100,000+ USD | Individual compassionate use or clinical trial only; high administrative burden; limited volume |
Note on costs: These ranges reflect the direct treatment costs (cell expansion, infusion, medical management) only. Total patient costs — including medical visa fees, flights, accommodation, translation services, and companion travel — should be factored into financial planning. For a full picture, speak with our coordination team through the contact page.
How to Access NK Cell Therapy in China
China Care handles the coordination process end-to-end for international patients. The process follows five steps.
Step 1: Submit Your Medical Records
Gather your complete oncology file: pathology report, staging workup (CT/PET-CT/MRI), blood work from the past 90 days, and a list of all prior treatments with dates and response data. Submit these through our contact page. China Care handles document translation and hospital pre-screening submission at no charge for initial evaluation.
Step 2: Hospital Matching and Pre-Screening
Based on your tumor type, treatment history, and goals, China Care identifies the most appropriate hospital program from our verified network — including PLA General Hospital Beijing, SAHZU Hangzhou, Shanghai Changzheng Hospital, SYSUCC Guangzhou, and Boao Lecheng programs. You receive a written pre-screening result within 2–3 weeks indicating whether you are likely eligible for trial enrollment or a non-trial program.
Step 3: Obtain a Medical Visa
China requires a specific medical visa (M-visa or referral letter from the treating hospital) for international patients accessing treatment. Our full guide on how to get a medical visa for China explains the current requirements, processing times, and documentation checklist for 2026.
Step 4: Travel and In-Country Arrival
On arrival at your destination city, China Care’s ground coordination team assists with airport transfer, hospital registration, translation support during consultations, and accommodation recommendations near the treatment facility. Companion coordination (visa support for a family member or caregiver traveling with you) is also available.
Step 5: Treatment and Follow-Up Coordination
During and after the treatment course, China Care maintains communication between you, your local oncologist at home, and the Chinese hospital team. Post-treatment follow-up documentation — response assessment reports, imaging summaries, and discharge summaries translated into English — is provided for sharing with your domestic care team.
To explore the full range of hospitals in our network across Chinese cities and specialties, visit our hospital directory.
FAQs
1. What is NK cell therapy, and how is it different from chemotherapy?
NK cell therapy uses living immune cells — your own or from a donor — to detect and kill cancer cells. Unlike chemotherapy, which attacks all rapidly dividing cells (including healthy ones) and causes systemic toxicity, NK cells are targeted by biology: they are specifically activated by signals of cellular stress and MHC-I downregulation on tumor cells. NK therapy aims to harness the immune system’s own recognition systems rather than using cytotoxic chemicals.
2. How is NK cell therapy different from CAR-T cell therapy?
Both are forms of cellular immunotherapy, but they work through different mechanisms and have different risk profiles. CAR-T cells are genetically engineered T cells designed to recognize a specific antigen on cancer cells — and they have produced transformative results in blood cancers (lymphoma, leukemia, multiple myeloma). NK cells are innate immune cells that work without prior antigen recognition, which makes them potentially useful against solid tumors where antigen heterogeneity limits CAR-T. NK cells also carry a lower risk of severe cytokine release syndrome and can often be used allogeneically (from a donor) without GvHD risk. However, CAR-T has a much stronger evidence base for blood cancers. NK therapy for solid tumors is at an earlier evidence stage. See our full CAR-T cell therapy in China guide for more on that modality.
3. Which solid tumors are being treated with NK cell therapy in China?
The most active research is in liver cancer (hepatocellular carcinoma / HCC), non-small cell lung cancer (NSCLC), gastric cancer, colorectal cancer, and nasopharyngeal carcinoma. Pancreatic cancer and ovarian cancer trials also exist. HCC currently has the most clinical data in the Chinese literature.
4. Is NK cell therapy approved or experimental?
NK cell therapy for solid tumors is investigational — it is not yet approved as standard of care in China, the United States, Japan, or Europe. In China, it is primarily conducted within registered clinical trials at academic medical centers, or through hospital-based research programs and the Boao Lecheng special regulatory zone. Patients should understand they are accessing investigational therapy, not approved standard-of-care treatment.
5. What are the main side effects of NK cell therapy?
Most patients experience mild-to-moderate side effects: fever, fatigue, and flu-like symptoms in the 24–48 hours following infusion are the most commonly reported. Serious adverse events directly attributable to NK infusion — severe CRS, neurotoxicity — are uncommon compared to CAR-T therapy, though they are not impossible. Side effects from any combination therapies (chemotherapy, anti-PD-1) are separate considerations.
6. How long do I need to stay in China for NK cell therapy?
Plan for at least one initial stay of 2–3 weeks for evaluation, NK cell expansion, and the first infusion course. Subsequent courses typically require stays of 1–2 weeks. Most complete programs involve 2–4 courses over 3–6 months. Travel from Southeast Asia and the Middle East is considerably less burdensome than from North America or Europe.
7. Can NK cell therapy be combined with my current treatment?
Potentially yes — many Chinese NK cell protocols are combination approaches pairing NK infusion with chemotherapy, anti-PD-1/PD-L1 checkpoint inhibitors, targeted therapy (sorafenib, lenvatinib for HCC), or interventional oncology procedures like TACE. The specific combination depends on tumor type, prior treatment history, and performance status. This is assessed during the hospital’s pre-screening and initial consultation process.
Start Your Consultation
NK cell therapy for solid tumors in China is an active, scientifically serious investigational option — and the access window, clinical trial availability, and cost advantages in China are significant for patients who qualify. China Care facilitates every step of the process, from medical record translation and hospital matching to in-country support and follow-up documentation.
Request a Free Medical Review
Submit your records and receive a written pre-screening assessment within 2–3 weeks.
Explore Our Hospital Directory
Browse our full network of verified oncology hospitals across China, with program details and specialties.
Read Our Cancer Treatment in China Guide
Compare the full range of solid tumor treatment options available through China Care — surgery, chemotherapy, targeted therapy, radiation, and immunotherapy.