China has become a global leader in CAR-T therapy for multiple myeloma, with Chinese institutions pioneering the GPRC5D target — now published in the New England Journal of Medicine — and offering CAR-T cell therapy in China at $80,000–$150,000 USD versus $465,000 in the United States. This guide explains who qualifies, which hospitals to consider, and how to access treatment through China Care Health Tours.
Key Facts
- BCMA CAR-T therapy for multiple myeloma costs $80,000–$150,000 USD in China versus $465,000 (Carvykti list price) or $420,000 (Abecma list price) in the United States as of 2026 — a 70–80% reduction.
- The CARTITUDE-1 trial reported a 97.9% overall response rate and 67% complete response rate for ciltacabtagene autoleucel (Carvykti) in patients with a median of 6 prior lines of therapy.
- A landmark 2022 Chinese Phase 1 study published in the New England Journal of Medicine reported 100% objective response rate in the highest dose cohort of GPRC5D-targeting CAR-T — the first clinical demonstration of this target’s potential.
- CAR-T manufacturing at Chinese centers takes 10–14 days, compared to 30–60 days for US commercial products — a clinically decisive advantage for patients with rapidly progressing disease.
- China is the global leader in GPRC5D-targeting CAR-T clinical experience — the only option for patients who have already failed BCMA-directed therapy (Abecma or Carvykti).
- GPRC5D CAR-T via Chinese clinical trials is available at $50,000–$100,000 USD — and some protocols significantly reduce patient costs further for trial-eligible patients.
- The NCCN guidelines now include anti-BCMA CAR-T as a Category 1 recommendation for relapsed/refractory myeloma after three or more prior lines of therapy.
Table of Contents
Why Multiple Myeloma Requires Advanced Treatment
Multiple myeloma is a cancer of plasma cells — the antibody-producing cells that live in bone marrow. Unlike many solid tumor cancers, myeloma is characterized by a relapsing-remitting pattern: most patients respond well to initial therapy, achieve remission, and then relapse. Each relapse is typically harder to treat than the last. With each successive line of therapy, responses become shallower and shorter.
Standard first-line treatment for myeloma typically combines a proteasome inhibitor (such as bortezomib or carfilzomib), an immunomodulatory drug (such as lenalidomide), and a steroid (typically dexamethasone) — often called a triplet regimen. For eligible patients, autologous stem cell transplantation (ASCT) is added after initial response. Anti-CD38 monoclonal antibodies like daratumumab have been added to standard regimens and substantially improved outcomes.
Despite these advances, myeloma remains incurable for the vast majority of patients. After three, four, or five lines of therapy, patients typically face a landscape where prior drug classes — proteasome inhibitors, IMiDs, anti-CD38 antibodies — have all been exhausted. This is called triple-class refractory or penta-refractory disease, and it carries a poor prognosis under conventional treatment.
CAR-T cell therapy represents a fundamentally different approach. Rather than administering a drug, physicians harvest a patient’s own T-cells, genetically engineer them to recognize and attack myeloma cells, expand them in a manufacturing facility, and infuse them back. This “living drug” can persist, proliferate, and hunt myeloma cells in ways conventional chemotherapy cannot.
For patients who have relapsed or progressed through multiple prior lines of therapy, CAR-T cell therapy in China has emerged as one of the most promising options available — and one of the most accessible in terms of cost and speed.
CAR-T Targets for Myeloma: BCMA, GPRC5D, and CD38
Not all myeloma CAR-T therapies are the same. The therapy’s effectiveness depends on the antigen — the molecular target on the surface of myeloma cells — that the engineered T-cells are programmed to attack. Three targets are now clinically significant: BCMA, GPRC5D, and CD38.
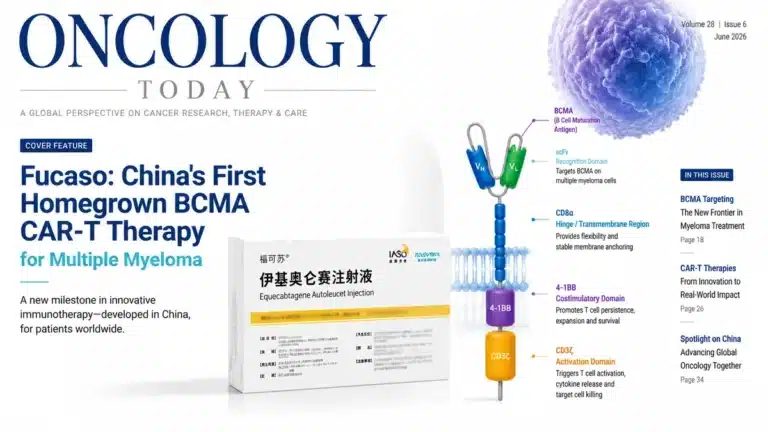
BCMA (B-Cell Maturation Antigen)
BCMA is expressed at high levels on the surface of myeloma plasma cells, making it the original and most established CAR-T target in this disease. The two FDA-approved CAR-T products for myeloma — idecabtagene vicleucel (Abecma, manufactured by Bristol Myers Squibb) and ciltacabtagene autoleucel (Carvykti, manufactured by Janssen/Johnson & Johnson) — both target BCMA.
In the United States, both Abecma and Carvykti are approved for relapsed/refractory myeloma after prior therapy. Carvykti, in particular, demonstrated strong efficacy in the CARTITUDE trial — 98% overall response rate in heavily pre-treated patients — and is now being evaluated in earlier lines of therapy.
Chinese institutions have been running BCMA CAR-T trials since 2017, preceding Western commercial approvals, and have treated hundreds of patients with domestically manufactured BCMA-targeting constructs. Chinese BCMA CAR-T products are manufactured locally — not shipped from US facilities — enabling faster turnaround and significantly lower cost.
GPRC5D — The Target China Pioneered
GPRC5D (G Protein-Coupled Receptor Class C Group 5 Member D) is expressed on myeloma cells and, critically, at minimal levels on normal tissues outside the bone marrow. This makes it an attractive target with a potentially favorable safety profile.
While GPRC5D had been studied in the laboratory, it was Chinese researchers who first demonstrated its clinical potential in CAR-T therapy. In 2022, a landmark study from Chinese hematologists was published in the New England Journal of Medicine — one of the world’s highest-impact medical journals — reporting remarkable response rates in relapsed/refractory myeloma patients treated with GPRC5D-targeting CAR-T cells, including patients who had previously failed BCMA-directed therapy.
This is critical for international patients: if you have received prior BCMA CAR-T therapy (such as Abecma or Carvykti in the United States) and have relapsed, GPRC5D CAR-T offers a second opportunity — targeting a different antigen that myeloma cells cannot simply downregulate to escape. Chinese centers are the global leaders in clinical experience with this target.
CD38
CD38 is the target of daratumumab (Darzalex), a standard-of-care monoclonal antibody in myeloma. CD38-directed CAR-T cells are being studied in China for patients who have progressed through anti-CD38 antibody therapy. While less mature than BCMA or GPRC5D programs, CD38-targeting CAR-T trials are active at several major Chinese hematology centers and represent the next generation of options for heavily pre-treated patients.
Bispecific CAR-T: Targeting Two Antigens Simultaneously
Several Chinese clinical programs are now evaluating bispecific or tandem CAR-T constructs that target both BCMA and GPRC5D simultaneously. The rationale: myeloma cells can escape single-target therapy by downregulating the target antigen. A bispecific construct makes this escape more difficult. Early data from Chinese centers are promising, and clinicaltrials.gov listings show multiple active studies recruiting internationally eligible patients.
Why China Leads in Myeloma CAR-T
China’s dominance in myeloma CAR-T is the product of three reinforcing advantages: scientific priority, regulatory environment, and cost structure.
Scientific Priority: The NEJM GPRC5D Publication
When researchers at Chinese institutions published the GPRC5D CAR-T myeloma data in the New England Journal of Medicine in 2022, it was not an incremental finding — it was the first demonstration that this target could achieve deep responses in patients who had no other options. Many of the patients in that cohort had already failed BCMA CAR-T therapy. The 100% overall response rate in that early cohort, though in a small number of patients, placed Chinese hematology on the world stage.
Western pharmaceutical companies have since begun developing their own GPRC5D-targeting products (talquetamab is a GPRC5D-directed bispecific antibody now approved in the US), but for CAR-T-specific GPRC5D therapy, Chinese centers have the deepest clinical experience. This is not a hypothetical advantage — it translates directly into physician expertise, nursing protocols, and CRS management experience.
Volume and Trial Access
China is currently running more cellular therapy clinical trials than any other country. Many of China’s leading hematology centers treat dozens of myeloma CAR-T patients per year, accumulating clinical experience far faster than Western academic centers where CAR-T volumes are constrained by commercial product availability, insurance approval timelines, and high cost. Chinese institutions offer both commercially available and trial-phase CAR-T products, including access to next-generation bispecific constructs not yet available anywhere else.
For cancer treatment in China, the combination of high volume, active research, and regulatory flexibility creates an environment where patients can access therapies at earlier stages than they could in Western healthcare systems.
Manufacturing Speed
One underappreciated advantage of Chinese CAR-T programs is manufacturing turnaround time. For BCMA CAR-T products in the United States, the vein-to-vein time (from leukapheresis to infusion) can exceed 30–60 days due to centralized manufacturing logistics. Several Chinese centers work with domestic manufacturers that can complete the CAR-T manufacturing process in 10–14 days. For myeloma patients with rapidly progressing disease, this speed can be clinically decisive.
Cost: Carvykti at $465,000 vs China at $80,000–$150,000
The most striking difference is cost. In the United States, Carvykti (ciltacabtagene autoleucel) has a list price of approximately $465,000 USD per infusion. Abecma (idecabtagene vicleucel) is priced at approximately $420,000. After bridging therapy, hospitalization, and infusion-related care, the total cost of BCMA CAR-T treatment in a US academic medical center commonly exceeds $500,000–$600,000.
In China, the equivalent BCMA CAR-T protocol — using domestically manufactured products with comparable response rates — is available at $80,000–$150,000 USD inclusive of manufacturing, hospitalization, and monitoring. GPRC5D CAR-T therapy, which is primarily accessed via clinical trial, may be available at further reduced cost for trial-eligible patients.
This 70–80% cost reduction is why an increasing number of US, Canadian, and UK patients with relapsed myeloma — particularly those without adequate insurance coverage for commercial CAR-T — are traveling to China for treatment.
Key Hospitals for Myeloma CAR-T in China
1. Institute of Hematology, Chinese Academy of Medical Sciences (CAMS) — Tianjin
The Institute of Hematology at CAMS in Tianjin is the premier blood cancer center in China and one of the most distinguished hematology institutions in Asia. It has been at the forefront of CAR-T development for hematologic malignancies since the earliest Chinese trials and has treated more CAR-T myeloma patients than most centers outside China. Its clinical research teams have published extensively on BCMA, GPRC5D, and bispecific CAR-T constructs. For patients seeking the deepest institutional experience with myeloma CAR-T, Tianjin CAMS is a leading option.
2. Peking Union Medical College Hospital (PUMCH) — Beijing
Peking Union Medical College Hospital is China’s most prestigious academic medical center, affiliated with Tsinghua University and CAMS. Its hematology department manages complex, multi-relapsed myeloma cases and has active CAR-T trial programs. PUMCH has English-speaking physician teams and significant experience managing international patients. Its multidisciplinary tumor board approach to myeloma — combining hematology, transplant, and cellular therapy — mirrors the standard of care at leading Western academic centers.
3. Ruijin Hospital, Shanghai Jiao Tong University School of Medicine — Shanghai
Ruijin Hospital‘s hematology department is internationally recognized, particularly for work on plasma cell disorders including myeloma and AL amyloidosis. Shanghai’s infrastructure for international patients — medical interpreters, international patient centers, proximity to Pudong International Airport — makes Ruijin a practical choice for patients traveling from Southeast Asia, Australia, or the Americas. Shanghai also offers the logistical advantage of direct flights from over 40 international destinations.
4. Gobroad Hospital — Beiing & Shanghai
Gobroad Hospital’s hematology network is one of China’s most specialized clinical research platforms for bone marrow transplantation and advanced cellular therapies, managing complex relapsed and refractory blood cancers including leukemia, lymphoma, and myelodysplastic syndromes. Its medical team is highly experienced in conducting cutting-edge CAR-T clinical trials, exploring novel multi-target designs alongside established therapies. With state-of-the-art flagship centers positioned directly in Beijing and Shanghai, Gobroad serves as the primary, highly connected international gateway for patients requiring specialized, research-driven hematology care.
5. Sun Yat-sen University Cancer Center (SYSUCC) — Guangzhou
SYSUCC is consistently ranked among China’s top three cancer hospitals. While its primary strength is solid tumor oncology — including nasopharyngeal carcinoma, for which it is a world reference center — its hematology-oncology program handles plasma cell malignancies, and its breadth of cancer specialties is invaluable for myeloma patients who may require concurrent management of extramedullary disease or other complications. SYSUCC’s international patient department has experience coordinating care for patients from over 50 countries.
You can review the full hospitals directory for additional certified hematology centers across China, including centers in Beijing, Zhengzhou, Wuhan, and Chengdu.
Who Qualifies for CAR-T Myeloma Therapy
CAR-T therapy is not appropriate for all myeloma patients. Eligibility is determined by a combination of disease history, performance status, organ function, and prior treatment history. The following table summarizes standard criteria, though individual centers may apply slightly different thresholds.
| Eligibility Factor | Typical Requirement |
|---|---|
| Prior lines of therapy | At least 3 prior lines, including a proteasome inhibitor, an IMiD, and an anti-CD38 antibody (triple-class refractory); some trial protocols accept 2 prior lines |
| ECOG Performance Status | 0–2 (ambulatory, capable of self-care) |
| Cardiac function | LVEF ≥ 45–50% (CAR-T cytokine toxicity can stress the heart) |
| Renal function | Creatinine clearance ≥ 40–45 mL/min (some protocols are more flexible) |
| Liver function | AST/ALT ≤ 3× upper limit of normal; bilirubin ≤ 2× upper limit |
| Pulmonary function | No severe active pulmonary disease; O2 saturation ≥ 92% on room air |
| Prior autologous SCT | Prior ASCT is acceptable and does not disqualify; prior allogeneic SCT requires longer time off immunosuppression |
| Prior BCMA-directed therapy | Prior BCMA CAR-T or bispecific antibody does not disqualify for GPRC5D-targeting programs — this is a critical pathway for relapsed patients |
| Active CNS myeloma | Active CNS involvement typically excludes standard CAR-T protocols; discuss with treating team |
| Active infection | Active uncontrolled infection must be treated before CAR-T; HIV-positive patients can be evaluated on a case-by-case basis |
Patients who do not meet all standard criteria should not self-exclude. Chinese centers have experience evaluating borderline cases, and trial protocols may have different thresholds. The first step is always a full case review by the treating hematology team.
The Treatment Process: Step by Step
Understanding the logistics of CAR-T therapy helps patients plan their travel, accommodation, and support arrangements. The process from initial evaluation to completion of monitoring typically spans 6–10 weeks.

Step 1: Case Review and Consultation (1–2 weeks, remote)
Before traveling, patients submit their full medical records — pathology reports, bone marrow biopsy results, imaging, treatment history, and most recent labs — for review by the Chinese hematology team. China Care Health Tours coordinates this process, arranging translation and secure submission of documents. The physician team provides a preliminary eligibility assessment and, if positive, a formal treatment proposal with cost estimate.
Step 2: Arrival and Pre-Treatment Evaluation (3–5 days)
Upon arrival in China, patients undergo comprehensive baseline evaluation: repeat bone marrow biopsy (to characterize active disease and confirm target antigen expression), full laboratory workup, cardiac assessment, and imaging. Patients requiring bridging therapy to control disease prior to leukapheresis may begin this during the evaluation phase.
Step 3: Leukapheresis (1 day)
Leukapheresis is the procedure by which T-cells are extracted from the patient’s blood. A large-bore IV or apheresis catheter is placed, and blood is passed through an apheresis machine that separates and collects the T-cells. The process takes approximately 3–5 hours and is performed as an inpatient or outpatient procedure.
Step 4: CAR-T Manufacturing (10–14 days)
The collected T-cells are sent to the manufacturing facility, where they are genetically engineered to express the CAR construct (targeting BCMA, GPRC5D, or other antigens), expanded to the required dose, quality-tested, and released. Chinese domestic manufacturers have reduced this turnaround to 10–14 days for many products — significantly faster than US commercial manufacturing. During this period, patients may remain in China or, in some cases, return briefly and come back for infusion.
Step 5: Lymphodepletion Chemotherapy (3 days)
Approximately 5–7 days before infusion, patients receive a short course of lymphodepletion chemotherapy (typically fludarabine and cyclophosphamide). The purpose is to reduce the number of the patient’s existing immune cells, creating “space” for the infused CAR-T cells to expand and engraft. This is administered as a brief inpatient admission.
Step 6: CAR-T Infusion (1 day)
The CAR-T infusion itself is a relatively straightforward intravenous administration, typically completed within 30–60 minutes. It takes place in a specialized hematology unit equipped for intensive monitoring.
Step 7: Monitoring and CRS Management (14–21 days)
The weeks following infusion are the most medically intensive. As the engineered T-cells expand and attack myeloma cells, they release inflammatory cytokines — a phenomenon called cytokine release syndrome (CRS). CRS can range from mild (fever, fatigue) to severe (hypotension, hypoxia). Chinese hematology centers with high CAR-T volumes have experienced teams and ICU backup for CRS management. Patients remain hospitalized for a minimum of 14–21 days post-infusion.
Step 8: Recovery and Follow-Up (2–4 weeks outpatient)
After hospital discharge, patients continue outpatient monitoring for 2–4 additional weeks before returning home. Follow-up blood tests, bone marrow biopsy (typically at Day 28–30 post-infusion), and imaging are used to assess response.
What the Evidence Shows
BCMA CAR-T: Established Efficacy
The clinical evidence for BCMA-targeting CAR-T in myeloma is now extensive. The CARTITUDE-1 trial, which evaluated ciltacabtagene autoleucel (Carvykti) in patients with a median of 6 prior lines of therapy, reported an overall response rate of 97.9% and a complete response rate of 67%. Median progression-free survival was approximately 35 months — a transformative result for patients who, by definition, had exhausted conventional options.
The KarMMa trial for idecabtagene vicleucel (Abecma) similarly reported ORR of 73% across dose levels, with deeper responses at higher doses and a median progression-free survival that, while shorter than Carvykti, represented significant improvement over prior expectations for triple-class refractory disease.
Chinese BCMA CAR-T programs have published comparable response rates in domestic trial populations. The NCCN guidelines for myeloma now include anti-BCMA CAR-T as a Category 1 recommendation for relapsed/refractory disease after three or more prior lines.
GPRC5D CAR-T: The Landmark Chinese Data
In 2022, the New England Journal of Medicine published results from a Chinese Phase 1 trial of GPRC5D-targeting CAR-T cells. The cohort included patients with heavily pre-treated relapsed/refractory myeloma, including patients who had previously received BCMA-directed therapy. In the highest dose cohort, 100% of evaluable patients achieved an objective response, including complete responses, in an early cohort of patients. Responses were observed even in patients who had already relapsed after BCMA CAR-T therapy — validating the mechanistic hypothesis that GPRC5D represents a non-overlapping escape pathway.
It is important to be honest about what the data does and does not show. The initial NEJM cohort was small, and long-term durability data is still maturing. Larger follow-up studies are ongoing at Chinese centers. Response rates — particularly for deeply pre-treated, BCMA-refractory patients — are compelling. Whether these responses translate into multi-year durable remissions at rates comparable to BCMA CAR-T in earlier-line disease is a question the field is still answering.
For patients with no remaining conventional options, particularly those who have already failed BCMA CAR-T therapy, the risk-benefit calculus clearly favors exploring GPRC5D-directed treatment.
Bispecific and Next-Generation Programs
Several Chinese centers are enrolling patients in trials of bispecific BCMA/GPRC5D CAR-T constructs, dual-target CD38/BCMA constructs, and armored CAR-T designs with enhanced persistence. These programs represent the true frontier of myeloma cellular therapy and are accessible to international patients through China Care’s trial matching service.
Cost Comparison: China vs USA, UK, and Singapore
The cost differential between myeloma CAR-T therapy in China and Western countries is one of the most striking in all of medical tourism. The table below reflects 2026 estimates.
| Country / System | BCMA CAR-T Product | Approximate Total Cost (USD) | Notes |
|---|---|---|---|
| United States | Carvykti (Janssen) | $500,000–$600,000 | Includes $465K list price + hospitalization, bridging, monitoring |
| United States | Abecma (BMS) | $450,000–$550,000 | Includes $420K list price + ancillary care |
| United Kingdom | Via NHS clinical trial | Trial-subsidized; private: £350,000–£450,000 | NHS access is trial-limited; private access is expensive |
| Singapore | Commercial / trial | SGD $500,000–$700,000 (~USD $370K–$520K) | Limited commercial availability; trial access is narrow |
| China — BCMA CAR-T | Domestic products | $80,000–$150,000 | Includes manufacturing, hospitalization, and 30-day monitoring |
| China — GPRC5D CAR-T | Trial programs | $50,000–$100,000 | Some trial protocols significantly reduce patient costs |
| China — Bispecific CAR-T | Trial programs | $60,000–$120,000 | Cost varies by protocol and institution |
These figures are estimates for planning purposes. Actual costs depend on the specific product, length of hospitalization, bridging therapy requirements, and individual patient complexity. China Care Health Tours provides detailed, itemized cost proposals after case review.
Cost must always be considered alongside the full picture of value: physician experience, institutional CAR-T volume, access to specific targets (particularly GPRC5D for BCMA-refractory patients), and trial access to next-generation constructs.
How to Access CAR-T Therapy for Myeloma in China
Step 1: Submit Your Medical Records
Send your complete medical file to China Care Health Tours through our secure intake process. This includes: pathology reports, bone marrow biopsy results (with immunohistochemistry showing BCMA/GPRC5D expression if available), full treatment history (all prior lines, dates, responses, and reason for discontinuation), most recent labs (CBC, CMP, SPEP/UPEP, free light chains, LDH), and any imaging. Our team will review for completeness before forwarding to the hematology specialist.
You can start this process through our contact page.
Step 2: Remote Physician Consultation
Our partner hematologists review your case and provide a preliminary eligibility assessment. For patients who are potentially eligible, the physician prepares a formal treatment plan including recommended CAR-T target (BCMA, GPRC5D, or bispecific), estimated timeline, and itemized cost estimate. This remote consultation typically completes within 5–7 business days.
Step 3: Visa and Travel Planning
China requires a medical visa (M-visa or JW201/JW202 visa) for patients traveling specifically for treatment. China Care assists with the medical visa application for China — including the hospital invitation letter required for the application. We also arrange airport transfer, accommodation near the hospital (often hospital-affiliated or partner guesthouses), and interpreter services for the duration of your stay.
Step 4: Arrive and Begin Evaluation
Upon arrival, you proceed through the pre-treatment evaluation phase described above. Our on-the-ground coordinator accompanies you to key appointments during the first week, ensuring communication is clear and medical decisions are fully understood. We work with the hospital’s international patient department to streamline paperwork, consent processes, and billing.
Step 5: Treatment, Monitoring, and Departure Planning
After infusion and the in-hospital monitoring period, our team coordinates discharge planning, arranges the outpatient follow-up schedule, and supports your return home with complete medical documentation for handover to your home oncologist. We remain available for questions and coordination throughout the post-treatment follow-up period.
China Care Health Tours is a medical facilitation service — we do not provide medical advice, and all clinical decisions are made by the treating physician team. Our role is to ensure that the logistical, linguistic, and coordination barriers that typically prevent international patients from accessing leading Chinese hematology centers are removed.
For patients already exploring CAR-T therapy for autoimmune disease in China as a separate indication, the process is broadly similar — if you are researching both indications for different family members, we can coordinate both inquiries simultaneously.
FAQ
What is the difference between BCMA CAR-T and GPRC5D CAR-T for myeloma?
BCMA (B-Cell Maturation Antigen) and GPRC5D are two different proteins expressed on the surface of myeloma plasma cells. BCMA was identified first and is the target of the two FDA-approved CAR-T products — Abecma and Carvykti. GPRC5D is a newer target, and its clinical potential was first established by Chinese researchers whose 2022 New England Journal of Medicine publication showed deep responses in relapsed/refractory patients. GPRC5D CAR-T is particularly relevant for patients who have already received BCMA-directed therapy, since it targets a different antigen — meaning myeloma cells cannot escape using the same mechanism as BCMA downregulation.
Can I receive GPRC5D CAR-T in China if I already received Carvykti or Abecma in the United States?
Yes. Failure of prior BCMA-directed CAR-T therapy does not disqualify you for GPRC5D-targeting programs. In fact, several Chinese clinical trials specifically enroll patients who have progressed after BCMA CAR-T — this patient population was represented in the landmark NEJM 2022 paper. Eligibility will depend on your current disease status, organ function, and time since prior CAR-T, but prior BCMA CAR-T therapy is not a disqualifying factor for GPRC5D-directed treatment.
How long do I need to stay in China for myeloma CAR-T therapy?
Plan for a minimum of 6–9 weeks in China. This includes the pre-treatment evaluation (approximately 1 week), CAR-T manufacturing waiting period (10–14 days), lymphodepletion and infusion, and the mandatory post-infusion hospital monitoring period (14–21 days). After hospital discharge, most programs require 2–4 additional weeks of outpatient follow-up before clearance to travel internationally.
What are the main risks of CAR-T therapy for myeloma?
The two primary toxicities are cytokine release syndrome (CRS) and immune effector cell-associated neurotoxicity syndrome (ICANS). CRS occurs as engineered T-cells expand and release inflammatory cytokines; it ranges from fever and fatigue (Grade 1–2) to severe hemodynamic compromise (Grade 3–4). ICANS, which can cause confusion, encephalopathy, or seizure, is less common with myeloma CAR-T than with lymphoma programs but is monitored carefully. Chinese centers with high CAR-T volumes have experienced teams managing both toxicities. All patients require inpatient monitoring for a minimum of 14 days post-infusion.
Is myeloma CAR-T covered by insurance for international patients?
Coverage varies significantly by country and insurer. US patients with commercial insurance may have partial or full coverage for FDA-approved products (Abecma, Carvykti) administered domestically, but coverage for treatment abroad is typically excluded. Canadian provincial health plans, UK NHS, and most Southeast Asian public health systems do not cover overseas CAR-T. Private travel health insurance does not typically cover elective medical treatment. Most international patients who travel to China for myeloma CAR-T are paying out of pocket, which is why the $80,000–$150,000 cost differential relative to US pricing is clinically and financially significant. We recommend consulting your insurer and a financial counselor before making a decision.
Does multiple myeloma stage affect CAR-T eligibility?
CAR-T is most commonly used in relapsed/refractory settings — typically after three or more prior lines of therapy. The stage at initial diagnosis (ISS I, II, or III) matters less than current disease activity, organ function, and prior treatment history. High-risk cytogenetics (del 17p, t(4;14), t(14;16)) do not necessarily exclude a patient but are part of the risk-benefit discussion — patients with high-risk disease may respond initially but have shorter progression-free survival. The treating physician will assess these factors as part of the eligibility evaluation.
What happens if I relapse after CAR-T therapy in China?
Relapse after CAR-T therapy — while disappointing — does not foreclose future options. Patients who achieve a deep response before relapsing may be eligible for another line of targeted therapy. Salvage options in China include retreatment with a different CAR-T target (e.g., GPRC5D CAR-T after BCMA relapse), bispecific antibody therapy, additional lines of proteasome inhibitor or IMiD-based regimens, or enrollment in a clinical trial for a next-generation cellular therapy. Our team remains available to discuss salvage options if a patient experiences disease progression after treatment in China.
Start Your Consultation
CAR-T therapy for multiple myeloma in China offers internationally competitive response rates at 70–80% lower cost than the United States — with unique access to GPRC5D-targeting programs pioneered by Chinese hematologists. Whether you are exploring initial CAR-T options or have already received BCMA-directed therapy abroad and are looking for next-line options, China Care Health Tours can coordinate your case review with leading Chinese hematology centers.